Published on
Differential Diagnosis
- ST-elevation myocardial infarction (STEMI)
- Left ventricular hypertrophy (LVH)
- Right bundle branch block (RBBB)
- Incomplete right bundle branch block (iRBBB)
- Left bundle branch block (LBBB)
Diagnosis
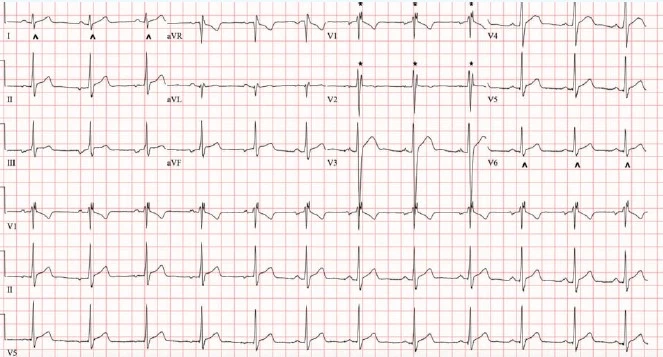
The diagnosis in this case is incomplete right bundle branch block. The ECG reveals a regular rhythm at a rate of 70 beats per minute. There is a normal axis. The axis of the p wave appears to be different in the first 5 beats, likely from an ectopic atrial focus, whereas the remaining beats appear to be sinus. The QRS complex duration is between 100-110 msec. There is an rSR’ pattern in V1-V2 and a wide/slurred S wave in the lateral leads (I, V6). The RBBB morphology with a QRS duration less than 120 msec indicates the presence of an incomplete right bundle branch block. There are no signs of ischemia.
Discussion
With a right bundle branch block, conduction through the right bundle is compromised, while the left bundle is unaffected. As the ventricles depolarize, conduction passes through the left bundle normally, across the left ventricle and through the myocardium to depolarize the right ventricle. Electrocardiographically, this creates a normal appearing early part of the QRS followed by a second R-wave (R’) in the anterior precordial leads, and a slurred S-wave in lateral leads as the conduction moves slower through the right ventricle.1 This slower-than-normal conduction results in a wide QRS (greater or equal to 120 msec). RBBB can be caused by a variety of problems including ischemia, fibrosis, calcifications, infiltrative disease, electrolyte disturbance, or impaired vascular supply.
Alternatively, an incomplete right bundle branch block has the same morphology as a right bundle branch block but with a QRS duration less than 120 msec. It is relatively common, especially in young people and males, but can affect people of all ages. One study on Swiss military conscripts with a mean age of 19 found an iRBBB prevalence of 13.%.2 While a RBBB has many dangerous causes, causes of iRBBB are most commonly benign. Often, iRBBB in the young, healthy population results from exercise-induced right ventricular remodeling and increased right ventricular free wall thickness, especially in athletes doing endurance exercise.
Because iRBBB is rarely pathologic, the clinical context is important to consider. Rare causes of iRBBB are structural abnormalities like atrial septal defect or conduction defects like Brugada syndrome or pre-excitation. In cases with a negative personal and family history and normal physical exam, iRBB does not need further evaluation. However, if abnormalities are found on clinical exam, a transfer should be initiated to further evaluate for cardiac disease.2
What to Look For
- RBBB is defined by RSR’ in V1 or V2, S-wave of greater duration than R-wave or 40ms in leads I and V6, andQRS duration greater than or equal to 120 msec.
- An incomplete RBBB shares the same morphology as a RBBB, but with a QRS duration less than 120ms.
Pearls for Initial Management, Considerations for Transfer
- Incomplete right bundle branch block is typically benign but should be interpreted in the clinical context.
- A patient with iRBBB and a negative personal and family history for cardiac disease, as well as a normal physical exam, does not need further evaluation.
- Patients with an iRBBB and abnormalities on clinical exam that could be related to cardiac disease should be transferred to a hospital for cardiology consultation and an echocardiogram.
References
- Surawicz B, Childers R, Deal BJ, Gettes LS. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram. Part III: Intraventricular Conduction Disturbances A Scientific Statement From the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. J Am Coll Cardiol.
- Kobza R, Cuculi F, Abächerli R, Toggweiler S, Suter Y, Frey F, et al. (December 2012). Twelve-lead electrocardiography in the young: physiologic and pathologic abnormalities. Heart Rhythm. 9 (12): 2018–2022.
- Floria M, Parteni N, Neagu AI, Sascau RA, Statescu C, Tanase DM (June 2021). Incomplete right bundle branch block: Challenges in electrocardiogram diagnosis. Anatolian Journal of Cardiology. 25 (6): 380–384.
Download the article PDF: 16-Year-Old With History Of Orchiopexy