Published on
Differential Diagnosis
- Hypocalcemia and hyperkalemia
- Third degree heart block
- Digoxin toxicity
- Atrial flutter
Diagnosis
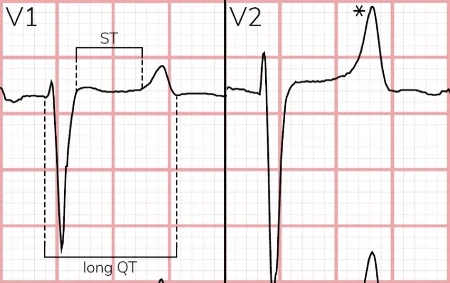
The diagnosis in this case is hypocalcemia, hyperkalemia, left ventricular hypertrophy. Therhythm is sinus with a ventricular rate of 70 beats per minute. There are large amplitude QRS complexes across the precordium consistent with left ventricular hypertrophy. There is QT prolongation and a peaked T wave morphology that suggests both hypocalcemia and hyperkalemia.
Discussion
Hypocalcemia characteristically increases the duration of the plateau phase of the cardiac action potential, manifesting as increased length of the ST-segment (Figure 2).1,2 This form of QT prolongation is unique and distinctly different than the delayed repolarization phase experienced during hypokalemia or with QT-prolonging medications. The presence of peaked T waves also suggests hyperkalemia. Electrocardiographic findings of hyperkalemia tend to follow a progression as toxicity progresses. Often, the earliest finding is narrow-based, peaked T waves (ie, pointed on top). At the extreme end of the hyperkalemia spectrum, sine wave morphology is a harbinger of impending ventricular fibrillation. 3–5
The combination of electrocardiographic findings of hypocalcemia (ie, lengthened ST-segment) and hyperkalemia (ie, peaked T waves) is a classic manifestation of end-stage renal disease. Risk factors for hyperkalemia include renal disease and medications like potassium-sparing diuretics, angiotensin converting enzyme inhibitors, angiotensin receptor blockers, and digoxin.
Patients with characteristic findings of hyperkalemia on electrocardiography should be immediately transferred to the nearest emergency center capable of dialysis by calling emergency medical services. As a temporizing measure, consider nebulizing albuterol (available in most urgent cares) to promote intracellular potassium shifting while awaiting transfer. This patient’s total calcium level was 5.2 mg/dL, and the potassium level was 6.5 mEq/L.
What to Look For
- Narrow-based, peaked T waves are often the earliest sign of hyperkalemia
- Prolonged QT by way of ST-lengthening is a unique manifestation of hypocalcemia
- The combination of ECG changes of hyperkalemia and hypocalcemia is classic for end-stage-renal disease
Initial Management, Considerations for Transfer
- Patients with electrocardiographic findings of hyperkalemia should be immediately transferred to the nearest emergency center capable of dialysis
- Consider 10-20 mg of nebulized albuterol as a temporizing measure while awaiting transfer
- If available, intravenous calcium can help stabilize the cardiac membrane when there are electrocardiographic changes of hyperkalemia, particularly QRS widening
- Consider placing automated defibrillator pads while awaiting transport
References
- Nijjer S, Ghosh AK, Dubrey SW. Hypocalcaemia, long QT interval and atrial arrhythmias. BMJ Case Rep. 2010;2010:bcr0820092216. doi:10.1136/bcr.08.2009.2216
- Bradley TJ, Metzger DL, Sanatani S. Long on QT and low on calcium. Cardiol Young. 2004;14(6):667-670. doi:10.1017/S1047951104006134
- Durfey N, Lehnhof B, Bergeson A, et al. Severe Hyperkalemia: Can the Electrocardiogram Risk Stratify for Short-term Adverse Events? Western Journal of Emergency Medicine. 2017;18(5):963-971. doi:10.5811/westjem.2017.6.33033
- Diercks DB, Shumaik GM, Harrigan RA, Brady WJ, Chan TC. Electrocardiographic manifestations: Electrolyte abnormalities. Journal of Emergency Medicine. 2004;27(2):153-160. doi:10.1016/j.jemermed.2004.04.006
- Mattu A, Brady WJ, Robinson DA. Electrocardiographic manifestations of hyperkalemia. Am J Emerg Med. 2000;18(6):721-729. doi:10.1053/AJEM.2000.7344
Download the Article PDF: 35-Year-Old With ESRD