ECG Differential Diagnosis
- Left ventricular hypertrophy
- Hyperkalemia
- ST-Elevation MI (STEMI)
- Early repolarization (ER)
- Pericarditis
Diagnosis
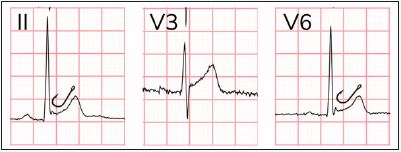
This patient was diagnosed with early repolarization (ER). This ECG reveals a sinus rhythm of 60 beats per minute, with a normal axis and normal intervals. There are mild, concave ST-elevations, most prominent in the precordium, and to a lesser extent the inferior leads. The ST-elevations are proportional to the amplitude of the QRS complex. There are no ST depressions or T-wave inversions. Additionally, J-point notching with a “fishhook” appearance can be seen, particularly in V6 (Figure 2). The combination of these findings is consistent with (benign) early repolarization.
ER has traditionally been considered a benign condition, but newer data suggest that its prevalence is higher among patients with idiopathic ventricular fibrillation. It is unclear, however, whether this finding has any significance among asymptomatic individuals.1 Because of this, nomenclature has shifted from benign early repolarization to, simply, early repolarization or the J wave pattern.
Electrocardiographic features of ER include diffuse ST elevations that are most pronounced in the precordial leads (typically V2-5) and in proportion to the amplitude of the QRS complex. The degree of ST elevation in V6 should be less than 25% the height of the QRS (greater than 25% suggests pericarditis).2 J point notching (ie, “fishhook”) can be seen (Figure 2). The T waves should be concordant (same direction as QRS), and there should not be any reciprocal changes to suggest myocardial infarction.3 When the diagnosis is in doubt, a calculator to help differentiate ER from a subtle anterior ST-elevation myocardial infarction may be useful.4
Current guidelines do not recommend direct treatment or other specific action to be taken for patients diagnosed with ER who have not experienced cardiac arrhythmias, syncope, or cardiac arrest. While individuals with ER seem to be at higher risk of ventricular fibrillation compared with the general population, the absolute risk is still extremely small.1 These patients can be safely discharged.
Learnings/What to Look for
- Electrocardiographic features of ER include:
- Diffuse ST-elevations that are most pronounced in the precordial leads (typically V2-5)
- The degree of ST elevation should be less than 25% the height of the QRS
- J point notching (ie, fishhook)
- Concordant T waves
- Absence of reciprocal changes to suggest myocardial infarction
Pearls for Urgent Care Management
- Utilize the clinical history in conjunction with the ECG to identify acute coronary syndrome
- No specific action needs to be taken for patients diagnosed with ER. They can be safely discharged
References
- Haïssaguerre M, Derval N, Sacher F, et al. Sudden cardiac arrest associated with early repolarization. N Engl J Med. 2008;358(19):2016-2023.
- Ginzton LE, Laks MM. The differential diagnosis of acute pericarditis from the normal variant: New electrocardiographic criteria. Circulation. 1982;65(5):1004-1009.
- Wagner GS, Strauss DG. Marriott’s Practical Electrocardiography. 12th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2014.
- Driver BE, Khalil A, Henry T, et al. A new 4-variable formula to differentiate normal variant ST segment elevation in V2-V4 (early repolarization) from subtle left anterior descending coronary occlusion—adding QRS amplitude of V2 improves the model. J Electrocardiol. 2017;50(5):561-569.