Differential Diagnosis
- Sinus bradycardia
- Myxedema coma
- Pericardial effusion
- Complete heart block
- Hypokalemia
Diagnosis
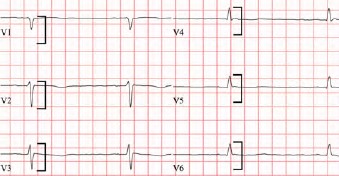
The diagnosis is myxedema coma. The ECG reveals sinus bradycardia with a rate of 40 beats per minute and low voltage. Atrial activity is difficult to see but careful analysis will reveal the presence of blunted P waves. There is also a prolonged QT interval. The traditional definition of low voltage is an amplitude less than 5 mm in the QRS complexes of all limb leads or an amplitude of less than 10 mm in the QRS complexes of all precordial leads.1 In this case, the patient had a QRS amplitude of less than 10 mm in all precordial lead (Figure 2).
The differential for low voltage can be broken down into two categories: cardiac abnormalities resulting in diminished impulse generation; and increased impedance due to attenuating substances between the heart and the surface leads (eg, fluid, air, or adipose tissue). Examples are in Table 1.
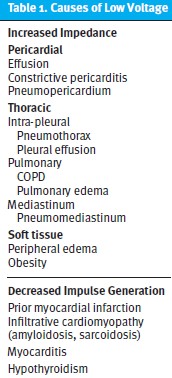
When low voltage is encountered, the provider must consider the listed conditions in the differential diagnosis. Many causes can be ruled out with a comprehensive physical examination (eg, obesity, peripheral edema) and ancillary testing as needed, such as chest x-ray (eg, COPD, pneumothorax) or bedside ultrasound when available (eg, pericardial effusion). Other conditions, such as hypothyroidism, are rarer and may require additional testing. The combination of low voltage and bradycardia should raise the concern for hypothyroidism/myxedema, as seen in this case.3 Concern for severe hypothyroidism or myxedema should trigger additional laboratory testing and/or transfer to higher level of care. Interestingly, hypothyroidism can cause low voltage through two mechanisms: the direct effects of hormonal deficiency on the generation of cardiac action potentials and via the presence of a pericardial effusion, seen in up to one-third of patients with hypothyroidism and, rarely, leading to tamponade.3,4 Patients with tamponade or large effusions due to hypothyroidism will characteristically lack a compensatory tachycardic response and will be bradycardic or normocardic.5,6 Other electrocardiographic findings of hypothyroidism include sinus bradycardia, low voltage, and prolonged QT interval. Occasionally, dysrhythmias like torsade de pointes can result.3,7 The presence of conducted P waves precludes the diagnosis of complete heart block. While hypokalemia can cause QT prolongation, it is not known to cause low voltage or bradycardia.
What To Look For
- Low voltage is caused by decreased impulse generation or increased impedance due to extracardiac causes like pericardial effusion, COPD, or obesity.
- Consider all causes of low voltage to avoid missing dangerous diagnoses.
- In patients with bradycardia and low voltage, consider hypothyroidism/myxedema coma.
Pearls For Initial Management, Considerations For Transfer
- Patients with severe hypothyroidism require transfer for admission, typically to an ICU.
- Be aware that hemodynamic instability could be caused by cardiac tamponade in patients with hypothyroidism, in which case fluid administration while preparing for immediate transfer is indicated.
References
- Madias JE. Low QRS voltage and its causes. J Electrocardiol. 2008;41(6):498-500. doi:10.1016/j.jelectrocard.2008.06.021
- Cooper BL, Giordano JA, Fadial TT, Reynolds CE. ECG Stampede: A Case-Based Curriculum in Electrocardiography Triage. 1st ed. (Cooper BL, ed.). Null Publishing Group; 2021.
- Danzi S, Klein I. Thyroid disease and the cardiovascular system. Endocrinol Metab Clin North Am. 2014;43(2):517-528. doi:10.1016/j.ecl.2014.02.005
- Tajiri J, Morita M, Higashi K, Sato T, Fujii H, Nakamura N. The cause of low voltage qrs complex in primary hypothyroidism pericardial effusion or thyroid hormone deficiency? Jpn Heart J. 1985;26(4):539-547. doi:10.1536/ihj.26.539
- Wang JL, Hsieh MJ, Lee CH, et al. Hypothyroid cardiac tamponade: Clinical features, electrocardiography, pericardial fluid and management. American Journal of the Medical Sciences. 2010;340(4):276-281. doi:10.1097/MAJ.0b013e3181e664c6
- Cooper BL, Ducach GJ, Fadial TT. Low and Slow. Ann Emerg Med. 2021;77(6):601-603. doi:10.1016/J.ANNEMERGMED.2020.12.010
- Wei Mak W, Nurazni Raja Azwan R, Badrulnizam Long Bidin M. Severe hypothyroidism presenting with supraventricular tachycardia. Med J Malasia. 2018;73(5):349-350.
Click Here to download the article PDF