Naushair Hussain, DO; Shahmeer Hussain, DO; Clinton A. Hartz, MD
Urgent Message: Scaphoid fractures most frequently occur at the mid aspect, or “waist,” of the scaphoid, and require about 10 weeks of prolonged immobilization before slow return to normal function. Such fractures have high risk of complications and subsequent chronic pain and/or disability if not appropriately immobilized.
Citation: Hussain N, Hussain S, Hartz C. Urgent Care Management of Scaphoid Fracture. J Urgent Care Med. 2024; 18(9):13-16
Editor’s Note: While the images presented here are authentic, the patient case scenarios are hypothetical.
Questions for the Clinician at the Bedside
- What mechanisms of injury are most likely to produce a scaphoid fracture?
- Why is it important to have a high index of suspicion for scaphoid fracture (even with negative wrist x-rays)?
- Which history and exam findings are concerning for scaphoid fracture?
- How should patients with ‘negative’ x-rays but concerning physical exam findings for scaphoid fracture be managed?
Clinical Scenario
A 56-year-old woman with no significant past medical history presents to the urgent care (UC) 3 hours after tripping and falling onto her outstretched hand (FOOSH). She complains of pain at the radial aspect of her left wrist, which is exacerbated with movement. She denies numbness or other injuries and has no neck, elbow, or shoulder pain.
On exam, the patient is noted to be holding her left hand in her lap in a guarded position. The left wrist is neither swollen nor showing deformity or bruising. However, there is tenderness to palpation that is most severe along the lateral aspect of the wrist and in the “anatomic snuffbox” and with axial loading of the thumb. The skin is intact and her neurovascular exam is normal.
A wrist x-ray is performed, which shows a transverse scaphoid fracture (Image 1).

The scaphoid fracture is the most common carpal fracture representing 90% of all cases.1 This most commonly results from a FOOSH mechanism of injury, but can also occur in contact sports.1 Scaphoid fractures more frequently occur at the mid aspect, or “waist,” of the scaphoid, and require about 6-10 weeks of prolonged immobilization before slow return to normal function.2 About 5-10% of cases occur at the proximal third, which takes 8-10 weeks to return to normal function, and 25% in the distal third with an average of 4-6 weeks of recovery.2
Up to one-quarter of patients presenting to an emergency department (ED) with wrist injuries where a scaphoid fracture is suspected (even with negative x-rays) will ultimately be diagnosed with scaphoid fractures.3 About 15% of scaphoid fractures are not visible on an initial plain x-ray.4 Due to the tenuous pattern of the bone’s blood supply, scaphoid fractures, radiographically apparent or occult, are at increased risk of nonunion, avascular necrosis, carpal collapse, and osteoarthritis if not appropriately immobilized.1,4
Relevant Anatomy
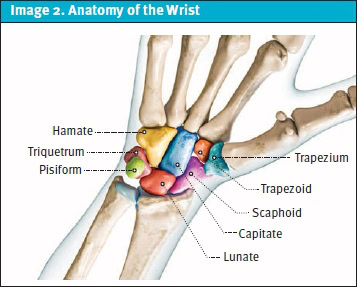
The 8 carpal bones of the wrist comprise 2 rows (distal and proximal), each consisting of 4 bones (Image 2). The scaphoid is the largest of the carpal bones in the proximal row. The majority of the scaphoid’s blood supply is through the dorsal carpal branch of the radial artery, which supplies the proximal 80% of the scaphoid’s blood supply through retrograde flow,2,5 The distal 20% of the scaphoid’s blood supply comes from the superficial palmar arch, which is a branch of the volar radial artery.2,5 As the blood flow to the scaphoid is primarily retrograde, an injury leaves the proximal portion of the scaphoid at high risk for avascular necrosis (AVN).1
The anatomic snuffbox is a triangular depression evident on the dorsal radial aspect of the wrist with extension of the thumb. The 3 edges of the triangle are the radial styloid at the proximal base, the extensor pollicis brevis tendon on the radial side, and the extensor pollicis longus tendon on the ulnar side. The floor is the scaphoid bone (proximal) and the trapezium bone (distal). It is important to palpate and document the presence of absence of snuffbox tenderness in patients presenting with wrist injury.
History
The history should focus on the timing and mechanism of injury. If a FOOSH has occurred, a scaphoid fracture should be suspected specifically when there is a history of pain on the radial side of the wrist after a high impact injury, which may have occurred on a hyperextended wrist.1 Pain with range of motion and other alleviating or exacerbating factors and the most precise location of the pain should be assessed as well as questions as to numbness, breaks in the skin, or other injuries.
Physical Exam
Examination begins with an inspection of the wrist for swelling. Gross deformity is rare with isolated scaphoid fracture and should raise suspicion of other wrist fractures. Neurovascular status should also be assessed, although gross derangements to neurovascular structures associated with scaphoid fracture are rare. Pain with resisted pronation and with circumduction of the wrist are concerning findings.1 Three additional tests to evaluate for suspected scaphoid fracture include the following, and a finding that all 3 tests are positive has a 74% specificity for a scaphoid fracture.2
- Tenderness with palpation at the anatomic snuffbox – Sensitivity: 96%, Specificity: 39%.3
- Scaphoid tubercle tenderness (assessed by extending the patient’s wrist and applying pressure to the tuberosity at the proximal wrist crease) – Sensitivity: 82-100%, Specificity: 17-57%.6
- Scaphoid compression test/axial compression of thumb (assessed by compressing the patient’s thumb along the axis of first metacarpal) – Sensitivity: 82%, Specificity: 58%.3
Radiographic Assessment
A stepwise approach to evaluation of the wrist x-rays will avoid missing important findings. When a scaphoid fracture is suspected, radiographic views should include posteroanterior (PA), lateral, semipronated oblique with the wrist in 45 degrees of pronation, semisupinated oblique with the wrist in 45 degrees of supination, and scaphoid views. The scaphoid view is taken with the wrist in 30 degrees of extension and 20 degrees of ulnar deviation.1
Look specifically at the scaphoid for:
- Breaks in the cortex
- Disruption in the trabeculation patterns
- Lucencies within the bone
- Angulation or impaction
- A “fat pad” sign on the radial aspect of the scaphoid bone.3
When X-rays yield negative results, the recommended advanced imaging modality for suspected scaphoid fractures is magnetic resonance imaging (MRI) of the wrist, which has a sensitivity of 96% and specificity of 98% for scaphoid fracture.3 When available, MRI during the initial assessment has been shown to be more cost-effective than immobilization followed by subsequent imaging.1,7,8,9 In cases where same-day MRI is unavailable (ie, most UC settings), wrist splinting until reassessment or MRI can be conducted is reasonable and appropriate. In cases where an MRI does not reveal abnormalities, patients are unlikely to derive significant benefit from cast immobilization and can thus commence earlier mobilization.2 It is recommended to conduct a follow-up clinical examination if symptoms persist without improvement within 3-4 weeks following initial injury.2
Management of Suspected Scaphoid Fracture in the Urgent Care
If no fracture is visible on radiographs of the wrist, but a fracture is clinically suspected, then the patient should be splinted in a rigid sugar tong with thumb spica.1,8,10 Avascular necrosis leading to nonunion and chronic pain is more common if fracture is initially not completely immobilized.1 Patients should follow up, ideally with an orthopedic specialist, and have repeat x-rays in 1-2 weeks to confirm whether evidence of fracture is apparent.4
When a fracture is identified on the initial radiographs, the next step involves determination of the pattern as stable or unstable then arrange rapid orthopedic follow-up. Stable fractures have a displacement of <1 mm, normal intercarpal alignment, and involve the distal pole. Unstable fractures are defined as >1 mm displacement, associated carpal bone angle instabilities, comminution, dorsal intercalated segmental instability, or involve the proximal pole. This classification is useful in determining whether patients will benefit from operative management.1
Nonoperative management is generally the preferred approach for fractures of the distal one-third and/or those that are minimally or nondisplaced (ie, stable).1 Patients are generally immobilized in a cast of the orthopedist’s choosing for 6-8 weeks. When operative management is pursued, percutaneous screw fixation or open reduction internal fixation are the common approaches orthopedists may implement.1
Return to sport needs to be individualized based on the type of activity and should be dictated by the orthopedist caring for the patient at follow-up. Patients can be given general guidance that at least 4 weeks, and up to 12 weeks, away from sport should be expected.1
Next Level Urgent Care Pearls
- Explore scaphoid fracture cases for other mechanisms of injury. If the injury occurred because of an altercation, consider injuries the patient may not be forthcoming about, including head or neck injury.
- When explaining the x-ray results to a patient, ensure they understand that a negative x-ray does not completely exclude a fracture.
- The advanced imaging test of choice for suspected scaphoid fractures with negative x-ray is an MRI scan of the wrist, which has a sensitivity of 96% and specificity of 98%.3
Red Flags and Legal Pitfalls
Data from 2 United Kingdom studies spanning roughly 1995-2012 on all litigation claims made as a result of wrist and scaphoid fractures found that reasons for litigation most commonly involved misinterpretation of x-rays, failure to immobilize, and delayed operative fixation.11 Approximately 74% of these litigation claims were settled resulting in a total payout of roughly $13 million (US).8 This highlights the importance of informing the patient that a negative x-ray does not exclude scaphoid fracture. Additionally, it is critical to examine the other carpal bones and their alignment for possible dislocation, as this represents a surgical emergency.
Clinical Scenario Conclusion
The patient had a wrist x-ray series that demonstrated a lucency across the mid aspect of the scaphoid, confirming diagnosis of scaphoid fracture. The patient was splinted in slight dorsiflexion with radial deviation in a sugar tong with thumb spica, and referred to an orthopedic specialist for follow-up in 3 days. The patient did follow up as instructed and the splint was changed to a cast. She was treated nonsurgically and immobilized for an additional 6 weeks, at which point the cast was removed with a good functional outcome.
Takeaway Points
- Scaphoid fractures are radiographically occult in 15% of cases and commonly occur with other serious wrist and forearm injuries. Evaluate the PA, oblique, and lateral radiographs, looking for additional fractures and/or dislocations, specifically for a carpal-metacarpal dislocation.
- Due to the tenuous blood supply of the scaphoid bone, the incidence of malunion and associated chronic pain and disability associated with missed scaphoid fractures is common.
- MRI, where available, is the preferred initial imaging modality to evaluate for suspected scaphoid fracture.
- If MRI is not available and there is tenderness over the anatomic snuffbox, scaphoid tubercle, and/or with axial loading of the thumb, the patients should be splinted as if there were a fracture, even if none is evident on x-ray.
- Proximal scaphoid fractures and those with >1mm of displacement are more likely to require surgical fixation.
Manuscript submitted May 14, 2024; accepted May 31, 2024.
References
- Li, Neill Y. MD; Dennison, David G. MD; Shin, Alexander Y. MD; Pulos, Nicholas A. MD. Update to Management of Acute Scaphoid Fractures. Journal of the American Academy of Orthopaedic Surgeons. 31(15):p e550-e560, August 1, 2023. | DOI: 10.5435/JAAOS-D-22-01210
- Clementson M, Björkman A, Thomsen NOB. Acute scaphoid fractures: guidelines for diagnosis and treatment. EFORT Open Rev. 2020 Feb 26;5(2):96-103. doi: 10.1302/2058-5241.5.190025. PMID: 32175096; PMCID: PMC7047900.
- Gemme S., et al, What physical examination findings and diagnostic imaging modalities are most useful in the diagnosis of scaphoid fractures? Ann Emerg Med. 2015; 65:308, March 2015
- Chaturvedi A, Russell H, Farrugia M, Roger M, Putti A, Jenkins PJ, Feltbower S. Patient-directed follow-up for the clinical scaphoid fracture. Bone Jt Open. 2024 Feb 9;5(2):117-122. doi: 10.1302/2633-1462.52.BJO-2023-0119.R1. PMID: 38330993; PMCID: PMC10853021.
- Almigdad A, et al. A review of scaphoid fracture, treatment outcomes, and consequences. International Orthopaedics. 2024:48(2), 529–536. https://doi.org/10.1007/s00264-023-06014-2
- Mallee WH, et al. Clinical diagnostic evaluation for scaphoid fractures: A systematic review and meta-analysis. Journal of Hand Surgery. 2014: 39(8), 1683-1691.
- Dean BJF, Little C, Riley ND, et al. Suspected scaphoid injuries managed by MRI direct from the emergency department: a single-centre prospective cohort study. Bone Jt Open. 2021;2(6):447-453. doi:10.1302/2633-1462.26.BJO-2021-0054.R1
- Ring J, Talbot C, Price J, Dunkow P. Wrist and scaphoid fractures: a 17-year review of NHSLA litigation data. Injury. 2015;46(4):682-686. doi:10.1016/j.injury.2015.01.017
- Rua T, et al. Cost-Effectiveness of Immediate Magnetic Resonance Imaging In the Management of Patients With Suspected Scaphoid Fracture: Results From a Randomized Clinical Trial. Value Health. 2020 Nov;23(11):1444-1452. doi: 10.1016/j.jval.2020.05.020. Epub 2020 Sep 29. PMID: 33127015.
- J. N., Ring D, CAST Trial Collaboration. Cast immobilization with and without immobilization of the thumb for nondisplaced and minimally displaced scaphoid waist fractures: a multicenter, randomized, controlled trial. J Hand Surg Am. 2014;39(4):621-627. doi:10.1016/j.jhsa.2013.12.039
- Harrison W, Newton AW, Cheung G. The litigation cost of negligent scaphoid fracture management. Eur J Emerg Med. 2015;22(2):142-143.
Download the article PDF: Urgent Care Management of Scaphoid Fracture
Author Affiliations: Naushair Hussain, DO, Indiana University School of Medicine. Shahmeer Hussain, DO, Adena Health System. Clinton A. Hartz, MD, Adena Health System. Authors have no relevant financial relationships with any ineligible companies.