What phenomenon explains the ST elevations in this ECG?
(Benign) early repolarization (BER) or the J wave pattern.
What are the features of this condition?
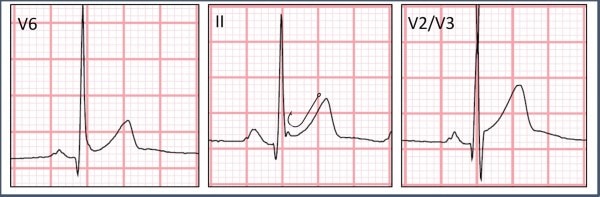
Features include diffuse ST elevations that are most pronounced in the precordial leads (typically V2-5) and in proportion to the amplitude of the QRS complex. The degree of ST elevation in V6 should be less than 25% the height of the QRS.1 J point notching (ie, “fishhook”) can be seen in Figure 2. The T waves should be concordant (same direction as QRS), and there should not be any reciprocal changes.2
What is the clinical significance of this phenomenon?
BER has traditionally been considered benign, but newer data suggest that the prevalence of the J wave pattern is higher among patients with idiopathic ventricular fibrillation. It is unclear, however, whether this finding has any significance among asymptomatic individuals.3
See the video provided by ECG Stampede for detailed analysis.
Pearls for Urgent Care Management
- Features of early repolarization include diffuse ST elevations that are most pronounced in the precordial leads (typically V2-5) with J point notching
- When early repolarization is recognized, there are no specific urgent care management recommendations
- If reciprocal changes or ST-segment convexity are present, or the patient presents with symptoms worrisome for acute coronary syndrome, transfer to a higher level of care is warranted
References
- 1. Ginzton LE, Laks MM. The differential diagnosis of acute pericarditis from the normal variant: new electrocardiographic criteria. Circulation. 1982;65(5):1004-1009.
- 2. Wagner GS, Strauss DG. Marriott’s Practical Electrocardiography. 12th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2014. 3. Haïssaguerre M, Derval N, Sacher F, et al. Sudden cardiac arrest associated with early repolarization. N Engl J Med. 2008;358(19):2016-2023.