Differential Diagnosis
- Left ventricular hypertrophy
- Hypertrophic cardiomyopathy
- Hypertension
- Aortic stenosis
- Body habitus

Diagnosis
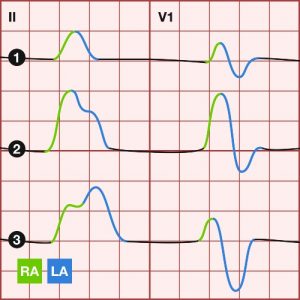
The correct diagnosis is body habitus. The ECG illustrates normal sinus rhythm at a rate of 96 bpm. There is rightward axis deviation (RAD) with positive deflections in II, III, and aVF with a nearly isoelectric QRS in lead I. The PR, QRS, and QT intervals are normal.
Evaluating for chamber enlargement, we note an increased amplitude P-wave in the inferior leads measuring between 2.5 and 3 mm. Right atrial abnormality (or enlargement) is identified with a P-wave amplitude of > 2.5 mm in lead II or >1.5 mm in V1/2.
Next, it is readily apparent that the QRS amplitudes are large—so much so that the peak in V4 extends well beyond the tracing paper. While this may increase the suspicion for left ventricular hypertrophy (LVH), several ECG criteria exist for a more definitive diagnosis:
- R wave in aVL >11mm
- S wave in V1 + R wave in V5/6 ≥35mm
- R wave in aVL + S wave in V3 >28 mm in males, or >20 mm in females
LVH is also commonly associated with some of the ST-segment and T-wave changes seen in this ECG, including the downsloping ST-segment depression and T-wave inversions most evident in V5/V6.
Learnings/What to Look for
Just as increased soft-tissue impedance from adipose or edema can influence the surface ECG by dampening the conduction of electrical impulses, an especially slender body habitus can have the inverse effect. In this case, the various electrocardiographic abnormalities were simply amplifications of normal cardiac activity. One potentially helpful hint is the combination of LVH with RAD—the former when truly representative of ventricular hypertrophy being more commonly associated with leftward axis deviation.
Key points
- Right atrial abnormality or enlargement: P-wave in II >2.5 mm or >1.5 mm in V1/2
- Left ventricular hypertrophy: R-wave in aVL >11 mm
- LVH repolarization changes include downsloping ST-segment depression and T-wave inversion
Pearls for Urgent Care Management
For asymptomatic or low-risk patients with slender body habitus and chamber abnormalities on ECG, outpatient follow-up is reasonable.
Resources
- Cooper BL, Giordano JA, Fadial TT, Reynolds CE. ECG Stampede: A case-based curriculum in electrocardiography triage. 1st ed. Houston, TX: Null Publishing Group, 2021.
- Harrigan RA, Jones K. ABC of clinical electrocardiography. Conditions affecting the right side of the heart. BMJ. 2002 May 18;324(7347):1201-1204.