The Resolution
Differential Diagnosis
- Normal sinus rhythm
- First-degree AV block
- Second-degree AV block
- Third-degree heart block
- Junctional bradycardia
- Sinus bradycardia
Diagnosis
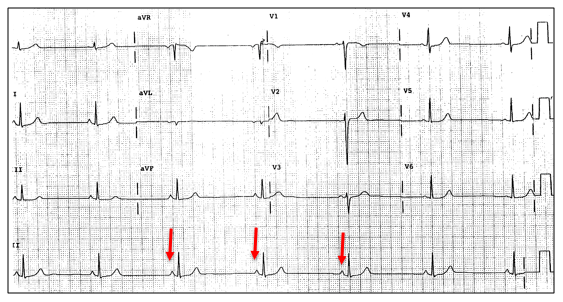
This ECG shows a sinus rhythm with a rate of 38. The normal rate is 60-100, so this is not simply a normal sinus rhythm.
The normal PR interval is 120-200 ms, and this PR is 155, which is normal; this is not first-degree AVB.
There is a P wave before each QRS and the PR interval is consistent; therefore, this is not second- or third-degree AVB.
Regarding the P waves: There are P waves before each QRS, so similarly this is not a junctional rhythm (where the depolarizing influence is from the AV node as opposed to the atrial node).
There are no T wave inversions concerning for ischemia; note that T wave inversions in aVR and V1 are normal. We do not see ST elevation or depression concerning for ischemia.
This ECG shows sinus bradycardia.
Learnings/What to Look for:
- The rate is normal (60-100), bradycardic (<60) or tachycardic (>100)
- With a very slow rate, consider heart block and ensure there is a P before each QRS and that there is not lengthening of the PR interval (Wenckebach) or a dropped QRS beat (Mobitz 2)
- Specifically evaluate each ECG for findings of ischemia such as T wave inversion or ST elevation or depression
Pearls for Urgent Care Management and Considerations for Transfer
- Sinus bradycardia is often an incidental finding, as in this case, and can occur as a normal variant or in athletes
- Compare to a previous ECG, if available
- Inquire if the patient is symptomatic including dizziness, weakness, fatigue, chest discomfort, shortness of breath, diaphoresis, hypotension or hypoxemia
- Medications such as beta blockers or calcium channel blockers may cause bradycardia as well as some electrolyte abnormalities. Inquire about meds in all patients. Lab testing should be individualized based on the providers pre-test estimation of risk
- Patients who are symptomatic should be emergently transferred to the emergency department