Differential Diagnosis
- Ectopic atrial rhythm
- Myocardial ischemia
- Myocardial infarction
- Limb lead reversal
Diagnosis
The ECG shows a regular, narrow-complex rhythm at a ventricular rate of 54 bpm. A QRS-complex follows every P-wave; however, the P-wave axis is abnormal—with an inverted P-wave in lead I and upright in aVR (where the inverse would be expected for sinus node origin). There are T-wave inversions in leads I and aVL, suggestive of myocardial ischemia.
This ECG illustrates a limb lead reversal (LLR).
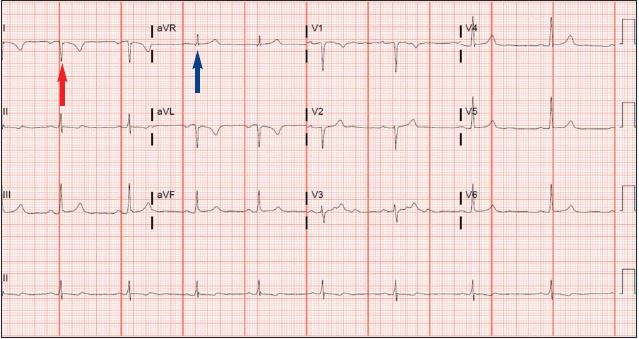
The presence of negative P-QRS complexes in lead I (red) is unusual for this young patient with no significant medical history. If the finding were to represent a real underlying condition (such as severe pulmonary disease), some corroboration in the precordial leads would be expected. Moreover, the bizarre positive P-QRS complexes in aVR (blue) suggest an alternative diagnosis—limb lead misplacement.
Between 0.4 and 4% of ECGs obtained in various settings demonstrate features of lead misplacement.1 Lead misplacement may either obscure important findings or simulate the appearance of ectopic rhythms, conduction disturbances, chamber abnormalities, and ischemia/infarction, resulting in unnecessary and potentially invasive testing.2
The key ECG findings suggestive of lead misplacement are dependent on the leads involved. The relationship between limb leads and surface electrodes are defined by Einthoven’s triangle (Figure 3).
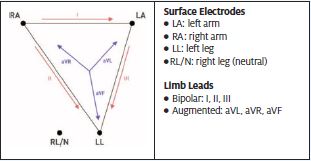
Limb lead reversals distort Einthoven’s triangle and result in predictable changes in the ECG3.
| Reversal | I | II | III | aVR | aVL | aVF |
| LA/RA | -I | III | II | aVL | aVR | – |
| LA/LL | II | I | -III | – | aVF | aVL |
| RA/LL | -III | -II | -I | aVF | – | aVR |
When lead reversals involve RL or the neutral electrode, a more dramatic distortion of Einthoven’s Triangle occurs such that one of the bipolar limb leads is conspicuously flat.
In this patient, the presence of negative P-QRS-T complexes in lead I combined with positive deflections in aVR are suspicious for LA/RA reversal. A repeat ECG was obtained (Figure 4).

Learnings/What to Look for
- Some key electrocardiographic features of limb lead reversal are:4-5
- Opposing directions of P-QRS complexes between I and V6 (limb and precordial leads with shared axes)
- Positive P-QRS in aVR
- Extreme axis deviation (between +180° and -90°)
- P-wave amplitude greater in lead I than II
- Very-low amplitude in isolated limb lead (I, II, III)
Pearls for Urgent Care Management
- Trust your clinical impression—a bizarre-appearing ECG with some of the features above warrants a repeat with careful attention to lead placement prior to definitive action
References
- Rudiger A, Hellermann JP, Mukherjee R, et al. Electrocardiographic artifacts due to electrode misplacement and their frequency in different clinical settings. Am J Emerg Medicine. 2007;25(2):174–178.
- Batchvarov VN, Malik M, Camm AJ. Incorrect electrode cable connection during electrocardiographic recording. Ep Europace. 2007;9(11):1081–1090.
- Harrigan RA, Chan TC, Brady WJ. Electrocardiographic electrode misplacement, misconnection, and artifact. J Emerg Medicine> 2012;4(3):1038–1044.
- Rosen AV, Koppikar S, Shaw C, Baranchuk A. Common ECG lead placement errors. part I: limb lead reversals. Int J Medical Students. 2014;2(3):92–98.
- Pérez‐Riera AR, Barbosa‐Barros R, Daminello‐Raimundo R, Abreu LC. Main artifacts in electrocardiography. Ann Noninvas Electro. 2018;23(2):e12494.
Acknowledgment: JUCM appreciates the assistance of ECG Stampede (www.ecgstampede.com) in sourcing content for electrocardiogram-based cases for Insights in Images each month.