Published on
Differential Diagnosis
- Lateral STEMI
- Wolff-Parkinson-White (WPW)
- Sinus tachycardia
- Brugada syndrome
- First-degree AV block
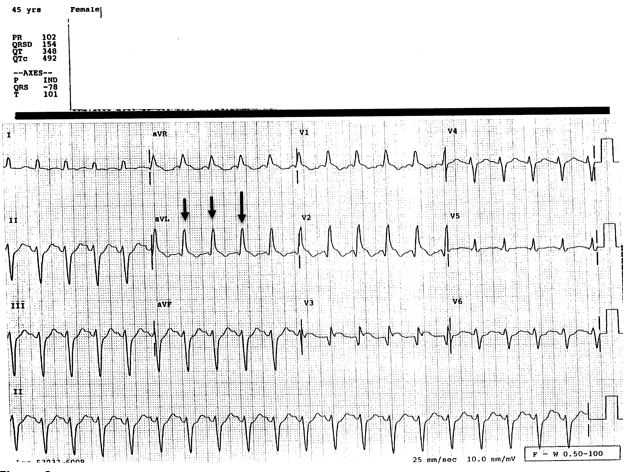
Figure 2.
Diagnosis
The ECG reveals a sinus tachycardia with a rate of 120.
The QRS is widened, and although a wide complex tachycardia should be evaluated for ventricular tachycardia, there are P waves before each QRS complex, so this is not V tach.
WPW can also cause a wide complex tachycardia with a short PR interval, but would show presence of the “upsloping” delta wave.
Brugada is an incomplete RBBB with ST elevation seen in leads V1 and 2, not present on this ECG. Normal PR interval is 0.12-0.20 and is not prolonged.
Other aspects of the ECG include bifascicular block as well as q waves anteriorly, likely indicating an old anterior MI.
There is ST elevation in leads V2 and V3; comparison to a previous ECG will help to determine if this acute from a STEMI or chronic.
Learnings/What to Look for
- Normal heart rate is 60-100 beats per minute
- Unexplained tachycardia, even in well-appearing patients, may indicate a more serious underlying process such as ischemia, myocarditis, aortic dissection, pneumothorax, pericardial tamponade, bleeding, or sepsis
- If the q waves and BBB are present on a previous ECG, this will help with the disposition decision by decreasing our concern; however, the tachycardia remains troubling for serious underlying pathology
- A smoker on oral contraceptive therapy over the age of 35 is at high risk for a thrombotic event such as pulmonary embolism (PE) or acute coronary syndrome (ACS)
Pearls for Initial Management and Considerations for Transfer
- A chief complaint of chest pain should prompt consideration of ACS, PE, and aortic dissection. Stratify risk based on the history of present illness and risk factors
- The presence of q waves in the above ECG is concerning for a previous MI. Though not 100% diagnostic, in the context of this presentation this should prompt consideration for emergent transfer
- Ongoing chest pain with an HPI concerning for ACS or PE should prompt emergent transfer, regardless of the ECG findings