Differential Diagnosis
- Myocardial infarction
- Left ventricular aneurysm
- Hypertrophic cardiomyopathy
- Wellens syndrome
- Brugada syndrome
Diagnosis
This patients was diagnosed with left ventricular aneurysm.
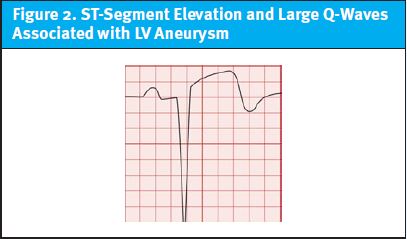
The ECG shows a normal sinus rhythm at a rate of 96 bpm. There is rightward axis deviation and intervals appear normal. Finally, there is ST-segment elevation in leads V2 and V3.
An acute myocardial infarction is always the leading concern for a patient with ST-segment elevation. In this case, the patient has no chest pain, and his symptoms are both subacute and mild. His presentation allows for a more comprehensive consideration of the differential for ST-segment elevation.
In this case, we note that the ST-segment elevations are preceded by large Q-waves. In the reported context of recent myocardial infarction. This is highly suggestive of a left ventricular aneurysm. (See Figure 2.)
In the absence of reperfusion therapy, left ventricular aneurysm is a common structural complication of acute myocardial infarction, occurring in 35% to 64% of patients with anterior acute myocardial infarction.1,2 Usual ECG findings of left ventricular aneurysm include ST-segment elevation that persists more than 2 weeks after STEMI, deep Q waves, and the absence of reciprocal ST-segment depressions. However, these features are neither sensitive nor specific for left ventricular aneurysm.3 The less-than-expected T-wave amplitude relative to the QRS can be quantified using “proportionality” formulae, further supporting the diagnosis of LV aneurysm. (See Table 1.)
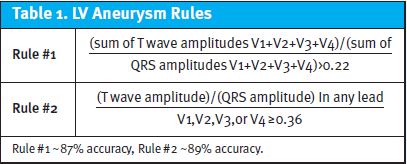
Importantly, neither rule’s test characteristics are sufficient to rule out ST-elevation myocardial infarction in a symptomatic patient.
Hypertrophic cardiomyopathy is the most common cause of sudden cardiac death among individuals under 40 years of age, and a cause of outflow obstruction. ECG findings include left ventricular hypertrophy, T wave inversions (especially in lateral leads), and narrow, “dagger” Q waves in the lateral leads (I, aVL, V5, V6).
Wellens syndrome is a syndrome of characteristic ECG findings—biphasic T waves (up then down) or deeply inverted and symmetric T waves in the anterior precordial leads V1-V3; in the correct clinical context that suggests a critical stenosis of the left anterior descending artery.
Brugada syndrome is a sodium channelopathy with a characteristic ECG pattern (ST segment elevation of ≥2 mm with a coved-type morphology in ≥1 right precordial lead) and an increased risk of sudden cardiac death, in the absence of gross structural heart disease.4
Learnings/What to Look for
While the differential diagnosis for ST-segment elevation is broad, immediate stabilization and management of myocardial infarction should be the priority for any patient with typical symptoms. In the context of recent myocardial infarction, it should be noted that left ventricular aneurysm, a delayed complication, can be associated with ST-segment elevation.
Key points to consider include:
- ST-segment elevation in precordial leads occurring >2 weeks after a myocardial infarction
- Associated with large Q-waves
- Low-amplitude T-waves identified visually or using “proportionality” formulae
Pearls for Urgent Care Management
This patient’s symptoms may be attributable to mild heart-failure. He warrants transfer for echocardiography to confirm the diagnosis of LV aneurysm suspected based on his ECG and identification of complications such as LV thrombus.
REFERENCES
- Mills RM, Young E, Gorlin R, Lesch M. Natural history of S-T segment elevation after acute myocardial infarction. Am J Cardiol. 1975;35(5):609-614.
- Meizlish JL, Berger HJ, Plankey M, et al. Functional left ventricular aneurysm formation after acute anterior transmural myocardial infarction. New Engl J Med. 1984;311(16):1001-1006.
- Klein LR, Shroff GR, Beeman W, Smith SW. Electrocardiographic criteria to differentiate acute anterior ST-elevation myocardial infarction from left ventricular aneurysm. Am J Emerg Med. 2015;33(6):786-790.
- Cooper BL, Giordano JA, Fadial TT, Reynolds CE. ECG Stampede: A Case-Based Curriculum in Electrocardiography Triage. 1st ed. (Cooper BL, ed). Null Publishing Group; 2021.