Differential Diagnosis
- Myocardial ischemia
- Congestive heart failure
- Myocarditis
- Conduction system disease
- Infiltrative (sarcoidosis, Lenègre-Lev)
- Infectious (bacterial endocarditis)
- Iatrogenic (valve replacement)
- Hyperkalemia
- Digoxin toxicity
Diagnosis
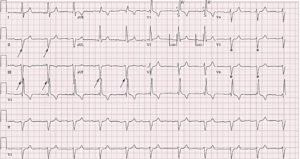
Right bundle branch block, left anterior fascicular block, first-degree AV block (trifascicular block). The ECG reveals a regular, wide-complex, sinus rhythm at a rate of 64 beats per minute. The PR-interval is prolonged (normal 120-200ms), indicating a first-degree atrioventricular block. The wide QRS complex (>120 msec), rSR’ appearance in V1, and wide S wave in the lateral leads (V5, V6, I, aVL) indicates the presence of a right bundle branch block. There is also an extreme left-axis deviation (>45⁰ deviation, indicated by a dominant S in the inferior leads II, III, aVF), which suggests an associated left anterior fascicular block.
Collectively, the findings of a right bundle branch block, left anterior fascicular block, and first-degree atrioventricular block suggest trifascicular disease or “trifascicular block.”
The term trifascicular block is a misnomer, as a true block of all three fascicles (the right bundle branch, left anterior fascicle, and left posterior fascicle) would result in complete heart block. Rather, the term references the presence of diseased conduction in all three fascicles with sufficient sparing of one fascicle (most commonly the left posterior fascicle), resulting in delayed conduction and manifesting as a prolonged PR interval (first-degree atrioventricular block). The American Heart Association guidelines suggest that use of the term “trifascicular block” be abandoned in favor of a description of the identified blocks independently (eg, right bundle branch block, left anterior fascicular block, first-degree AV-block).1
First-degree blocks are usually seen in active, healthy patients without heart disease. They typically represent a process within the atrioventricular node itself and are unlikely to progress to complete heart block. However, when accompanied by preexisting conduction disease (eg, right bundle branch block, left bundle branch block, or bifascicular block) they can indicate infranodal conduction disease.
Immediate referral to the emergency department is warranted when patients with significant conduction disease present with symptoms suggesting intermittent bradycardia (eg, syncope or presyncopal lightheadedness), as progression to higher degree blocks, including complete heart block, can occur. These patients should be evaluated for permanent pacemaker placement.2 The rate of progression to complete heart block in patients with multiple fascicle disease is approximately 1% per year.3
Learnings/What to Look for
Trifascicular block is a misnomer. ECG interpretation should instead describe the identified blocks. Traditionally, the term has referenced blocks involving
- Right bundle branch
- Left anterior or posterior fascicular block
- First-degree atrioventricular block
Pearls for Urgent Care Management and Considerations for Transfer
- Patients with multiple fascicle disease who are bradycardic or symptomatic with presyncope or syncope should be transferred to an emergency department immediately for evaluation
- These patients may need subsequent transfer to a facility with capability for permanent pacemaker placement after stabilization
- If multiple fascicle disease is identified in an otherwise asymptomatic patient (eg, ECG obtained for preoperative evaluation), a careful screening for signs or symptoms of occult cardiac disease should be performed; in some cases ambulatory electrocardiographic monitoring may be considered4
References
- Surawicz B, Childers R, Deal BJ, et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2009;53(11):976-981.
- Epstein AE, Dimarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;51(21):e1-62.
- McAnulty JH, Rahimtoola SH, Murphy E, et al. Natural history of “high-risk” bundle-branch block: final report of a prospective study. N Engl J Med. 1982;307(3):137-43.
- Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. J Am Coll Cardiol. 2019;74(7):932-987.
Acknowledgment: Images and case provided by Tom T. Fadial, MD.