Published on
Differential Diagnosis
- Left ventricular hypertrophy (LVH)
- Left bundle branch block (LBBB)
- Left anterior fascicular block (LAFB)
- Pre-excitation
- Inferior myocardial infarction (MI)
Diagnosis
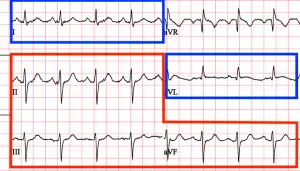
This patient was diagnosed with left anterior fascicular block. The ECG shows a sinus tachycardia with a rate of 102 bpm. There is a left axis deviation (to learn how this was visualized quickly, see Figure 2) with normal PR/QT intervals. There are no overt signs of ischemia.
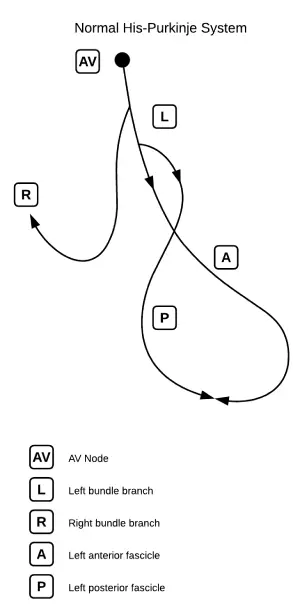
The His-Purkinje system is responsible for electrical conduction through the ventricles. During normal depolarization, a rapid electrical impulse travels through the ventricles and then splits into the right and left bundles. The left bundle branch is further subdivided into the anterior and posterior fascicles (Figure 3). Disruption of both fascicles produces a left bunch branch block, but each fascicle can be affected individually as well, producing either a left anterior fascicular block (LAFB) or left posterior fascicular block (LPFB).
When the left anterior fascicle is disrupted, current runs through the posterior fascicle to depolarize the left ventricle in a leftward and upward direction. This creates a left axis deviation. Alternatively, a left posterior fascicular block causes the left ventricle to depolarize in a rightward and downward direction, producing a right axis deviation.
In evaluating this patient’s ECG, we can see that there are no other causes of a left axis deviation. In the absence of left ventricular hypertrophy, left bundle branch block, pre-excitation, or inferior q waves, the cause of the leftward axis deviation is left anterior fascicular block.
Criteria for LAFB includes:
- Left axis deviation (usually -45° to -90°)
- Small q waves with large R waves in I and aVL (qR complexes)
- Small r waves with large S waves in II, III, and aVF (rS complexes)
- Normal or slightly prolonged QRS (80-110 ms)1
In isolation, LAFB is not clinically significant. When the LAFB is seen in combination with other conduction system disease (ie, a right bundle branch block or first-degree atrioventricular block), it may signal intermittent complete heart block, especially in a symptomatic patient.
Learnings/What to Look for
- When assessing an ECG with left axis deviation, run through the differential including left ventricular hypertrophy, left bundle branch block, left anterior fascicular block, pre-excitation, and inferior MI. This will help to identify cases of LAFB
- Consider the clinical context of the patient with conduction system disease
Pearls for Urgent Care Management
- Asymptomatic patients with LAFB do not require additional workup or treatment
- For patients with LAFB with another conduction delay (ie, RBBB, first-degree AV block, etc.), consider the patient’s presentation and symptoms. If the patient is symptomatic with syncope or presyncope, consider transfer for telemetry monitoring, echocardiography, and possible electrophysiologic evaluation
References
- Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2019;140(8):e382-e482.
- Surawicz B, Childers R, Deal BJ, et al. AHA/ACCF/HRS Recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association electrocardiography and arrhythmias committee, council on clinical cardiology; the American College of Cardiology foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2009;53(11):976-981.
Download the article PDF: A 61-Year-Old Female with History of Hypertension and New Palpitations and Shortness of Breath