ECG Differential diagnosis:
- ST-Elevation myocardial infarction (STEMI)
- Acute right heart strain
- Left ventricular hypertrophy (LVH)
- Ischemic T-wave inversions/Myocardial ischemia
- Hypertrophic cardiomyopathy
Diagnosis
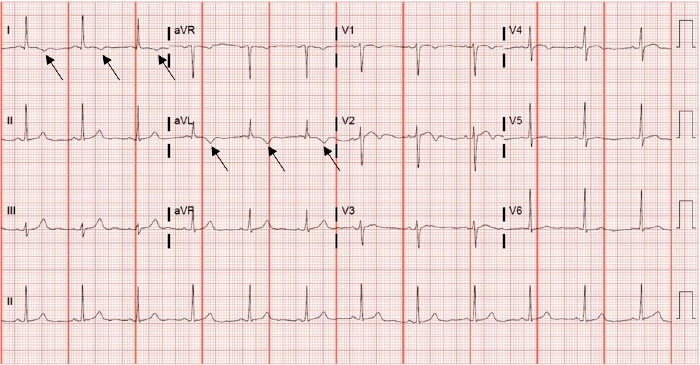
This patient was diagnosed with ischemic T-wave inversions/myocardial ischemia. The ECG reveals a sinus rhythm at a rate of 72 beats per minute. There is a normal axis and normal intervals. There are symmetric T-wave inversions in the high lateral leads (1, aVL), as well as a biphasic t-wave in V2. There are no ST elevations or depressions.
T-wave inversions in leads aVR and V1 are normal characteristics on the ECG, and an isolated T-wave inversion in lead III is a normal variant (“a flipped T is free in III”). Inverted t-waves can also be a normal finding in pediatric ECGs. New T-wave inversions when compared to old ECGs are always abnormal.
There are many causes of T-wave inversions, and ECG interpretation should occur within the clinical context of the patient’s presentation; our patient is presenting with symptoms consistent with acute coronary syndrome, and the finding of symmetric T-wave inversions in contiguous anatomical leads (lateral leads) is consistent with myocardial ischemia. Dynamic T-wave inversions on serial ECGs are typically seen with acute ischemia, whereas fixed T-wave inversions are seen after infarction and are often associated with pathologic Q-waves.1
Other causes of T-wave inversions include persistent juvenile T-wave pattern, normal repolarization changes after a bundle branch block, left ventricular hypertrophy, acute right heart strain as often seen in pulmonary embolism, hypertrophic cardiomyopathy, takotsubo cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy,2 and cardiac memory,3 as well as elevated intracranial pressure.
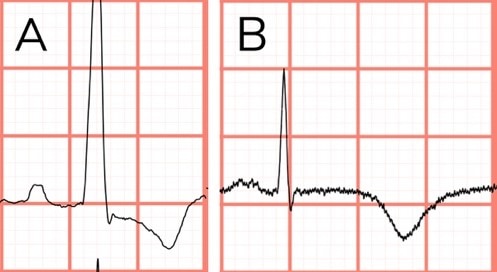
Distinguishing between ischemic T-wave inversions and T-wave inversions of ventricular hypertrophy is important for accurate diagnosis. Ischemic T-waves are found in contiguous leads and tend to be symmetric and deep, whereas T-wave inversions secondary to the “strain” of left ventricular hypertrophy are found in the lateral and high lateral leads (I, aVL, V5 and V6) and are asymmetric (Figure 3).4 ECGs consistent with the “strain” of left ventricular hypertrophy should also meet voltage criteria for the diagnosis.
Learnings/What to Look for
- The differential for T-wave inversions is broad and includes:
- Juvenile T-wave pattern
- Normal repolarization changes after a bundle branch block
- Left ventricular hypertrophy
- Acute right heart strain as often seen in pulmonary embolism
- Hypertrophic cardiomyopathy
- Takotsubo cardiomyopathy
- Arrhythmogenic right ventricular cardiomyopathy
- Cardiac memory
- Elevated intracranial pressure
- Normal in pediatric patients
- The correct interpretation of T-wave inversions relies on the clinical presentation
- Dynamic T-wave inversions on serial ECGs are consistent with acute ischemia in the setting of acute coronary syndrome.
- Differentiating between ischemic T-wave inversions and the strain pattern of ventricular hypertrophy is based on the morphology of the T-wave and voltage criteria of the QRS
Pearls for Urgent Care Management
- Utilize the clinical history in tandem with the ECG to identify the cause of T-wave inversion
- Serial ECGs, as well as comparison to prior ECGs, can help guide decision making
- In the setting of acute coronary syndrome, identification of acute ischemic T-wave inversions on ECG should prompt the provider to transfer the patient to a coronary intervention-capable facility
References
- Wagner GS, Strauss DG. Marriott’s Practical Electrocardiography. 12th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2014.
- Haugaa KH, Haland TF, Leren IS, et al. Arrhythmogenic right ventricular cardiomyopathy, clinical manifestations, and diagnosis. Europace. 2016;18(7):965–972.
- Polito SC, Giordano JA, Cooper BL. Cardiac memory-induced T-wave inversions. Clin Pract Cases Emerg Med. 2020 Apr 14;4(2):181-184.
- Wagner GS, Macfarlane P, Wellens H, et al. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram. Part V: Electrocardiogram Changes Associated with Cardiac Chamber Hypertrophy. Circulation. 2009;53(11):1003-1011.
View Similar Cases
- A 48-Year-Old Female With Months Of Fatigue, Nausea, And Body Aches—Including Chest Pain
- A 74-Year-Old Female With Multiple Episodes Of Chest Pain Over A 2-Day Period