Differential Diagnosis
- Diffuse subendocardial Ischemia
- Left ventricular hypertrophy (LVH) with strain
- ST-elevation myocardial infarction (STEMI)
- Non─ST-elevation myocardial infarction (NSTEMI)
- Wellens syndrome
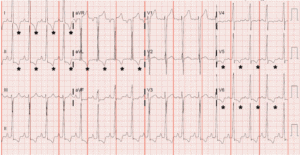
*Leads with “strain” pattern of ST-depressions and asymmetric t-wave inversions.
Diagnosis
This patient was diagnosed with left ventricular hypertrophy (LVH) with strain. The ECG reveals sinus tachycardia with a rate of 102 beats per minute, large amplitude QRS complexes, and prominent t-wave inversions primarily in the lateral leads (I, aVL, V5, V6). The morphology and distribution of the t-wave inversions are particularly important to note, as this distinction can help differentiate between more chronic, stable changes and acute changes that require more immediate attention.
Several electrocardiographic criteria exist for left ventricular hypertrophy, and none of them are particularly sensitive (~50%), but they are quite specific (85%–90%). Two of the more commonly cited criteria are shown below:
| Select Electrocardiographic Criteria for Left Ventricular Hypertrophy (QRS Amplitude) | |
| Sokolow-Lyon Criteria | S V1 + R V5,6 > 35 mm OR R aVL > 11 mm |
| Cornell Criteria | R aVL + S V3 > 28 mm for men OR > 20 mm for women |
Repolarization abnormalities are commonly associated with left ventricular hypertrophy, namely asymmetric t-wave inversions and ST-depressions that predominate in the lateral leads—the so-called “strain” pattern, as with this ECG. It is not uncommon to see discordant ST changes associated with LVH, meaning ST changes in the opposite direction as the QRS complex. Notice that ST-depressions are seen in leads with up-going QRS complexes (I, II, aVL, V5, V6), and ST-elevations are seen in leads with down-going QRS complexes (aVR, V1). In fact, while multi-lead ST-depression and aVR ST-elevation has been described as a pattern strongly associated with left main or triple vessel disease (ie, diffuse subendocardial ischemia), it is also commonly seen with LVH.
T-wave inversions can also indicate acute ischemia, but the t-wave inversions of acute ischemia tend to be symmetric. When deep and symmetric t-waves are seen in the anterior precordial leads while the patient is chest-pain free, it may indicate critical stenosis of the left anterior descending artery—Wellens syndrome (see figure below).
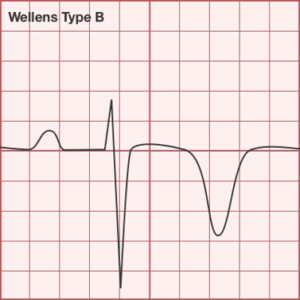
Image used with permission from ddxof.com.
While ST-elevations are seen in V1 and aVR, they do not represent STEMI. ST-elevations associated with STEMI are more commonly straight or convex upward in appearance (ie, “tombstone” morphology). If STEMI were the diagnosis, one would expect the presentation to be more acute, as opposed to 2 months of symptoms without an acute change. Most importantly, if an old ECG is available for comparison (as it was with this patient), one could confirm the unchanged presence of the ST/T changes. NSTEMI cannot necessarily be ruled out based on the ECG; it requires a rise and/or fall in serial cardiac biomarkers, but the subacute to chronic presentation is not consistent with NSTEMI.
Learnings/What to Look for:
- Electrocardiographic findings of LVH include large-amplitude QRS complexes (see text for definitions).
- LVH can be associated with repolarizations abnormalities including ST-depressions and asymmetric t-wave inversions in the lateral leads (I, aVL, V5, V6).
- When in doubt, compare to prior ECGs.
Pearls for Urgent Care Management and Considerations for Transfer
- If the patient is acutely symptomatic with either chest pain, shortness of breath, or with unstable vital signs (ie, hypoxia) then immediate referral to the emergency department is indicated
- If the ECG reveals classic LVH findings but the patient is not acutely symptomatic, consider blood pressure control as hypertension is the most likely culprit; however, acute control is not necessary
Acknowledgment: Images and case provided by Benjamin Cooper, MD, FACEP, assistant professor and associate program director, McGovern Medical School, Department of Emergency Medicine, The University of Texas Health Science Center at Houston.
