Published on
Differential Diagnosis
- Hyperkalemia
- Myocardial infarction with hyperacute T waves
- Myocarditis
- Hypocalcemia
- Brugada syndrome
Diagnosis
This patient was diagnosed with hyperkalemia due to acute renal failure.
ECG Analysis
This ECG shows a regular ventricular rate of 72 bpm without discernable P waves. The T waves are narrow-based with a pointed peak and the QRS is slightly widened. These findings are consistent with hyperkalemia.
Electrocardiographic findings of hyperkalemia tend to follow a progression as toxicity progresses (Table 1). Often, the earliest finding is narrow-based, peaked T waves, and at the extreme end of the hyperkalemia spectrum, a sine wave morphology is a harbinger of pending ventricular fibrillation.
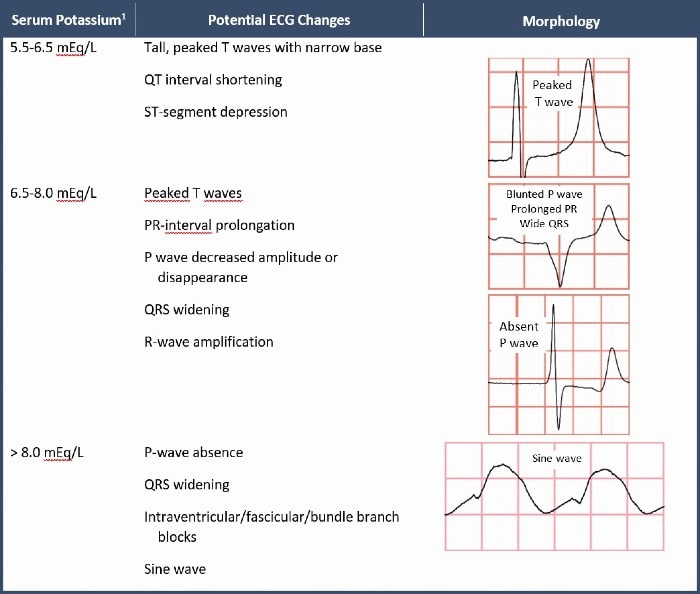
The ECG can be used to predict short-term hyperkalemic adverse events. According to one retrospective study of 188 patients with severe hyperkalemia, the following three findings predicted adverse outcomes within 6 hours:
- Bradycardia <50 bpm
- QRS >110 ms
- Junctional rhythm
Notice that peaked T waves were not found to predict acute adverse outcomes.2
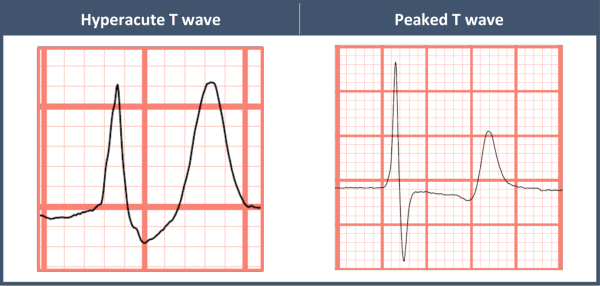
While other differential considerations exist, it is most important to differentiate hyperacute T waves from the peaked T waves of hyperkalemia.
Peaked T waves of hyperkalemia tend to be narrow-based with a pointed peak, as opposed to the broad base and rounded peak of hyperacute T waves (Figure 2).
Myocarditis can cause hyperacute T waves, but does not tend to cause peaked T waves.
Hypocalcemia can cause a prolonged QT interval by way of prolongation of the ST-segment.
Brugada syndrome is a sodium channelopathy with a characteristic ECG pattern (pseudo-right bundle branch block pattern with down-sloping ST segment elevation in V1 and/or V2) and an increased risk of sudden cardiac death, in the absence of gross structural heart disease.
Acute treatment of hyperkalemia includes membrane stabilizers like calcium and hypertonic saline, and intracellular potassium shifters like insulin, beta-agonists, and sodium bicarbonate.1 Patients with electrocardiographic features concerning for hyperkalemia should have all available treatments initiated and be transferred immediately to a dialysis-capable facility.
The potassium level in this case was 9.1 mEq/L, and the patient was immediately transferred to an emergency center for emergent dialysis.
Learnings/What to Look for
- Electrocardiographic features of hyperkalemia include peaked T waves, P wave blunting, and QRS widening
- ECG findings that predict short-term adverse outcomes include bradycardia less than 50 bpm, QRS width greater than 110 msec, and a junctional rhythm
Pearls for Urgent Care Management
- Any ECG features suggesting hyperkalemia should prompt initiation of available treatments and transfer to a dialysis-capable facility
- Nebulized albuterol is a simple and easily administered therapy in the urgent care setting that can be given while awaiting emergency transportation to shift potassium intracellularly
References
- Long B, Warix JR, Koyfman A. Controversies in management of hyperkalemia. J Emerg Med. 2018;55(2):192-205.
- Durfey N, Lehnhof B, Bergeson A, et al. Severe hyperkalemia: can the electrocardiogram risk stratify for short-term adverse events? Western J Emerg Med. 2017;18(5):963-971.