Published on
Differential diagnosis:
- Junctional bradycardia
- Atrial fibrillation
- Bradycardia with Wolff-Parkinson-White syndrome
- Brugada syndrome
- Third degree heart block
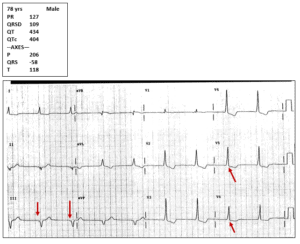
Diagnosis: The patient is experiencing bradycardia with Wolff-Parkinson-White syndrome (WPW).
Though this is a bradycardic rhythm, there is evidence of P waves before the QRS complexes (see downward arrows below at lead III), so it is not a junctional bradycardia (no P waves).
The rhythm is regular, and not irregularly irregular as in atrial fibrillation.
Brugada syndrome is important to recognize, as it may degrade into a terminal rhythm; it is diagnosed by the presence of incomplete right bundle branch block and ST elevation in leads V1 and V2, but is not present on this ECG.
Third-degree heart block results in a bradycardic rate, but usually with a rate in the 30s; additionally, in this ECG a P wave precedes the QRS complexes, while in third-degree (complete) heart block there is complete dissociation between the P waves and the QRS complexes.
This ECG shows bradycardia with WPW. Note the short PR interval and the upsloping “delta” waves in the V5 and V6 (upward arrows).
Learnings/What to Look for
- WPW is a supraventricular re-entrant rhythm
- Patients may be asymptomatic, with the WPW being found incidentally, or may include complaints of anxiety, palpitations, dizziness, chest discomfort, or shortness of breath
- ECG findings include a short PR interval, a delta wave (upsloping initial portion of the QRS complex), and a prolonged QRS complex
Pearls for Initial Management and Considerations for Transfer
- Compare to previous ECG if available
- If found incidentally, the patient does not require transfer and outpatient referral is appropriate
- The patient should be transported emergently to the emergency department via EMS if symptomatic with chest discomfort, shortness of breath, tachycardia, hypotension, hypoxemia, or altered mental status
- Note that WPW may occur with atrial fibrillation and reveal an irregular tachycardic rhythm with a wide complex QRS. Do not use calcium channel blockers, adenosine, beta blockers, or digoxin, as these may precipitate ventricular fibrillation and death. WPW may occur with atrial fibrillation is managed medically with procainamide or electrically with cardioversion