Urgent message: Recent expert opinion has reshaped initial management for suspected acute renal colic. Clinicians often utilize computerized tomography imaging to diagnose acute renal colic; however, there is an increasing role for clinicians to instead use point-of-care ultrasound (POCUS) as the initial imaging modality when acute renal colic is suspected. Renal ultrasound is time and cost effective, radiation-free and completed by the clinician at the bedside.
Chelsea M. Burgin, MD, FAAFP; James Frederick W. Pike, MSIII; and John Eicken, MD, EdM
INTRODUCTION
Acute pain from renal colic can be severe and debilitating. The presentation of an active stone causes agony for both the patient and kin. There is often a sense of urgency “to do something” beyond acute symptom management. Patient expectations resulting from Google searches, social media, or perceived standards of care may contribute to a clinician’s decision to order a CT. Although CT offers precise diagnostic detail, it has not been shown to significantly alter management for renal colic.1–3 In certain patient populations and clinical scenarios, POCUS serves a role as an alternative imaging modality to CT. POCUS has been shown to have a high positive predictive value for renal colic in the presence of hydronephrosis.4,5 POCUS is time- and cost-effective, completed at the bedside, lacks radiation, and can provide ample information to help direct care.
Clinical Scenario A—Presentation
A 38-year-old female presented to urgent care with waxing and waning right flank pain which radiated to her right groin for 7 days. She denied nausea and vomiting. Past medical history was significant for hypertension. She denied a personal and family history of renal stones. On presentation she was afebrile with a heart rate of 93 and blood pressure 174/102. On physical examination she had appeared to be in mild distress, no visible signs of trauma or rash, speaking comfortably, cardiopulmonary exam unremarkable; there was no abdominal tenderness although she had mild right costovertebral angle tenderness. Her urine dip was positive for blood.
Clinical Scenario B—Presentation
A 57-year-old male presented to urgent care with 6 hours of left flank pain with associated nausea and emesis. He reported a remote personal history of kidney stones. He did not have a primary care provider and had not sought medical care in over a decade. His oral temperature was 99.5⁰F with a heart rate of 105 and a blood pressure of 148/98. On physical examination he had tenderness in his left lower quadrant. His urine dip was negative for blood.
BACKGROUND Evaluation for patients with symptoms of acute renal colic commonly involves imaging with CT, ultrasound, or both. As a result of its diagnostic utility, the use of CT has vastly increased over the last 20 years. From 1996-2007, the use of CT increased 10-fold in patients presenting with suspected acute renal colic.1
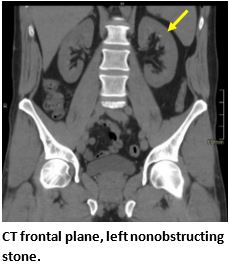
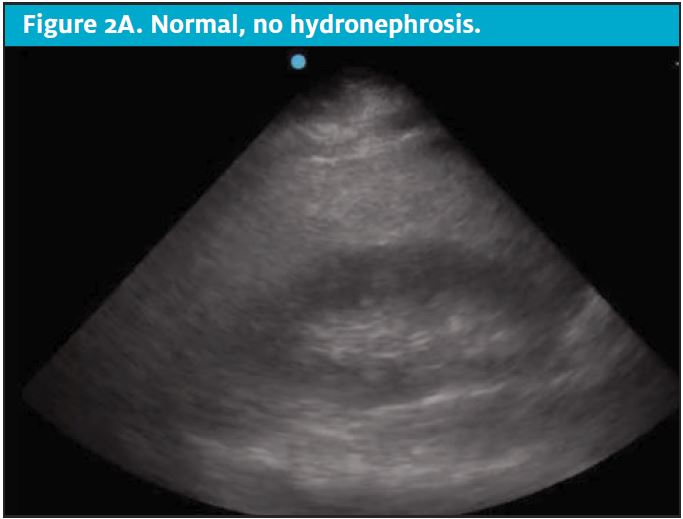
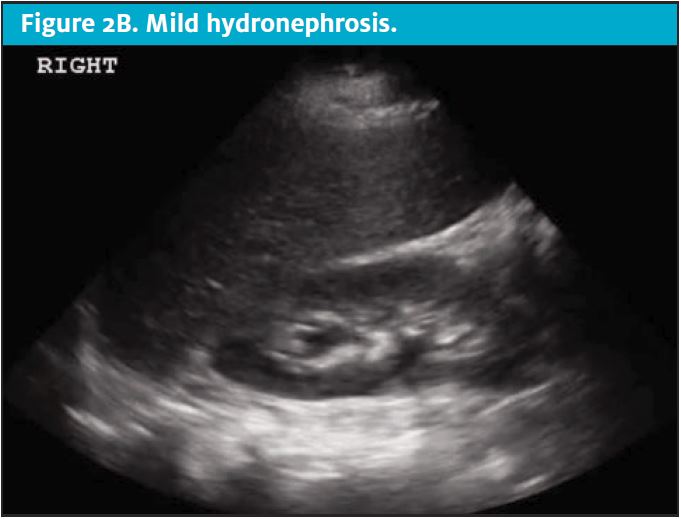
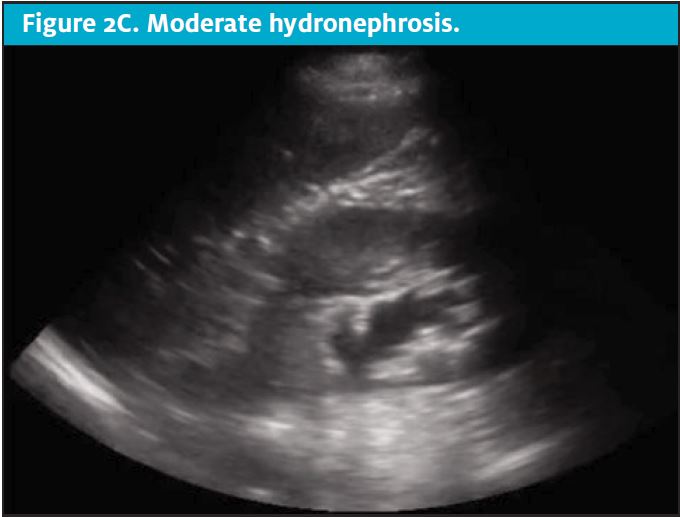
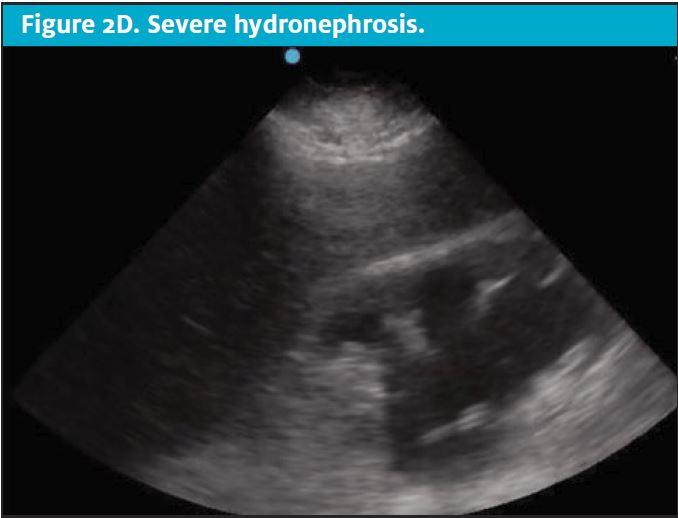
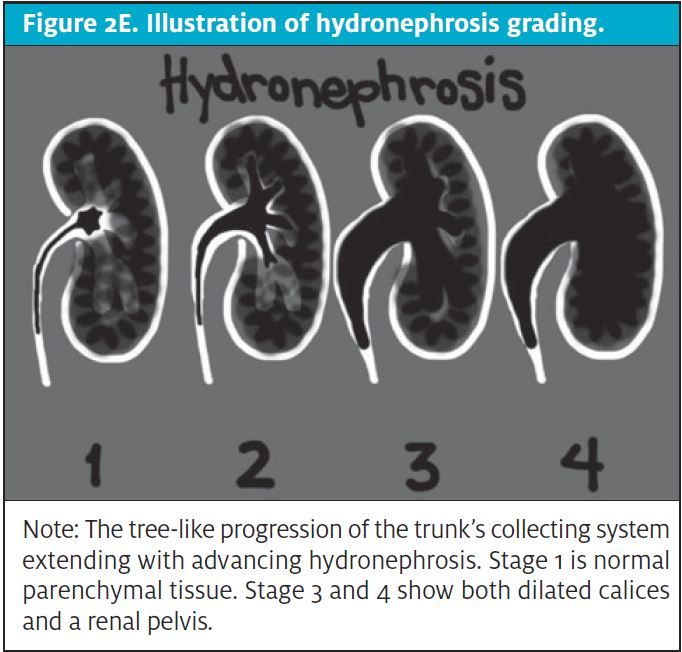
CT scans come at a high cost to the patient, both financially and through exposure to ionizing radiation.6,7 Unfortunately, patients with nephrolithiasis frequently have recurrence, leading to repeat imaging over time and further accumulation of radiation.8Clinicians should consider the carcinogenic effects of cumulative radiation when making decisions regarding advanced imaging for suspected acute renal colic. Limiting radiation exposure, especially in low-risk patients, is just one compelling reason to seek diagnostic alternatives to CT. Efforts are being made to implement imaging alternatives at a global level. As an effective alternative in low-risk patients, POCUS has been shown to effectively diagnose acute renal colic through the presence of moderate to severe hydronephrosis and can offer direct visualization of a ureteral stone at the ureterovesical junction.2,9 (See Figures 2A-2E.)
DISCUSSION
Prevalence of kidney stones is increasing. One international article highlighted the linear relationship of obesity and diabetes to renal stone incidence and prevalence.10 The National Health and Nutrition Evaluation Survey reported nephrolithiasis increasing in prevalence from 3.2% in 1980 to 10.1% in 2014.11
Ultrasound as the sole imaging modality for suspected renal colic increased from 2.6 to 6.5% between 2007 and 2015.12 Despite the increase, it reflects less than one-tenth the use of CT imaging. One study comparing emergency physician POCUS to radiology department ultrasound revealed no statistical difference in the confirmation of renal colic in the presence of moderate to severe hydronephrosis.13 Adopting renal POCUS for the assessment of hydronephrosis in certain populations with signs and symptoms of acute renal colic has the potential to reduce radiation, reduce expense for both the patient and hospital, increase patient satisfaction, and reduce ED visits. Furthermore, POCUS performed at the bedside during the initial evaluation is particularly relevant when CT imaging is not available.
With the prevalence of kidney stones increasing it is important to equip and prepare UC clinicians for the future. Renal POCUS can help clinicians achieve this goal as it is a noninvasive, brief bedside procedure effective at identifying sonographic signs of acute renal colic. UC clinicians who possess kidney and bladder POCUS skills can improve medical decision making in suspected renal colic.
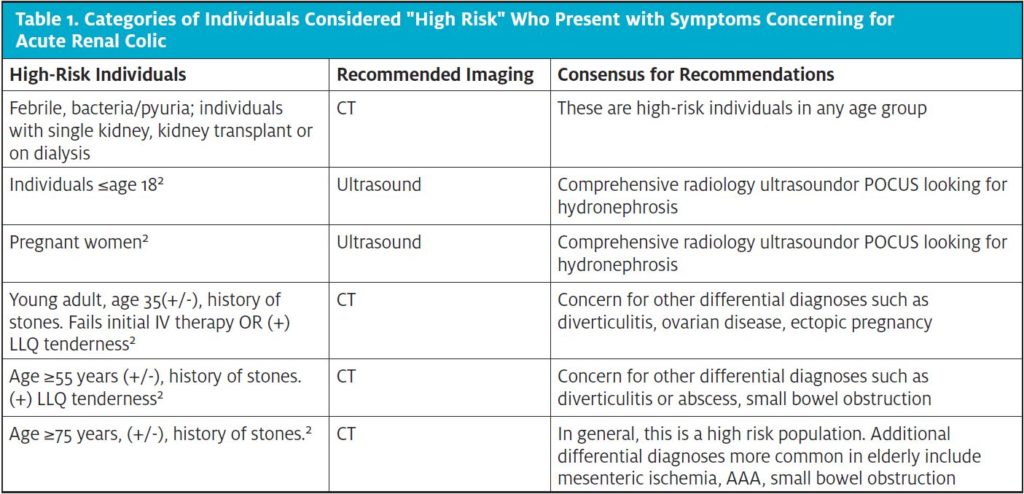
As is true for all POCUS applications, it is essential to ensure renal POCUS is being applied within the appropriate context. High-risk individuals in whom renal POCUS should not be the primary imaging modality include those who present with fever, pyuria concerning for infection, increased age with no history of nephrolithiasis, history of single kidney, current pregnancy, or history of kidney transplant. If the clinician has high concern for a more serious alternative diagnosis, then POCUS should not be the sole imaging modality. Finally, it is important to utilize the POCUS findings in a manner that aligns with evidence-based literature.
One multicenter comparative trial analyzed the value of POCUS compared to CT in suspected nephrolithiasis in 2,759 patients not identified as high risk between the ages of 18 and 76. These individuals were randomly assigned to undergo POCUS, ultrasound performed by radiology, or CT abdomen/pelvis. There were no significant differences between ultrasound and CT in the following variables: diagnostic accuracy, patient outcomes, serious or relative adverse events. Additionally, there was no significant difference between the CT and ultrasound groups in regards to the average pain score after seven days, incidence of high-risk diagnoses within 30 days, nor return visits or hospitalizations.8
Replacing CT imaging with ultrasound reduces radiation and expedites care in acute renal colic for low risk populations without negatively impacting outcomes. POCUS led to shorter length-of-stay when compared to radiology department performed ultrasound or CT. Time is an important factor to consider within the practice of urgent care medicine.
Practice Altering Advanced Imaging Multispecialty Agreement
In September 2019, nine experts from the specialties of emergency medicine, radiology, and urology gathered together to combine their clinical wisdom with evidence-based medicine to create a set of standard recommendations on imaging for patients who present with acute renal colic. Twenty-nine different scenarios were discussed, with preferred imaging modalities were voted on by each specialist. The end result included multispecialty guidelines to provide a framework for clinicians who evaluate individuals with suspected acute renal colic.2
The panel came to the agreement that no further imaging was needed in 13 of the scenarios, ultrasound was the best approach to imaging in nine of the cases, and CT was favored in seven of the scenarios.
The scenarios for which CT was considered the modality of choice included older patients (≥75 years), middle-age and older patients with no prior history of nephrolithiasis, patients who failed to respond to initial medical management, or those with atypical presentation without hydronephrosis on ultrasound and individuals with focal abdominal tenderness. This multidisciplinary panel confirmed that CT should be avoided in most patients age 35 or less, patients under 18 years old and in pregnant patients. It was also concluded that CT should be avoided in the middle-aged patient if there is a prior history of kidney stone unless features such as tenderness or lack of response to initial medical therapy were present. In summary, emergency medicine, radiology and urology were in agreement that ultrasound (POCUS or radiology performed) is an appropriate alternative to CT in a number of common clinical scenarios.
Clinical Scenario A—Conclusion
During her urgent care stay the patient received 1 L of normal saline, intravenous ketorolac, and ondansetron. A renal POCUS was performed and the clinician did not identify any hydronephrosis. Urine culture was obtained. Over the course of her stay, she experienced improvement in pain and nausea with modest improvement of her blood pressure. Given her improvement in addition to being considered “low-risk” she was discharged home with a urine strainer, ketorolac, and lisinopril and a diagnosis of suspected acute renal colic. Four days after the patient’s urgent care visit the clinician called the patient to inform her of the negative urine culture and to check on her. Her pain and nausea had completely resolved and she reported doing well. There was inconsistent use of urine strainer, although to her knowledge no stone was excreted. She had an appointment with a new primary care provider the following morning to reevaluate her blood pressure and current medications.
Clinical Scenario B—Conclusion
At the urgent care center he received 1 L of normal saline, intravenous ketorolac and promethazine. Limited renal POCUS was done and moderate hydronephrosis was seen. However, given his focal tenderness to palpation in the left lower quadrant in addition to his lack of response to initial IV therapy, the provider appropriately obtained CT imaging for further evaluation which later that day revealed the presence of both diverticulitis and a 4.5 mm renal stone in the distal ureter. He was treated outpatient with amoxicillin-clavulanate, promethazine, hydrocodone-acetaminophen, and a liquid diet. Two days after the patient’s urgent care visit the clinician called to check on him; the patient reported passing the stone that morning and his abdominal pain was significantly better. He was tolerating clear liquids and ready to advance to a semi solid diet.
CONCLUSION
In a patient with a history, physical examination, and/or laboratory results concerning for acute renal colic who is responsive to medical management with the exclusion of high risk individuals, the literature favors avoidance of CT. Moderate or severe hydronephrosis identified on renal POCUS greatly increases the likelihood of acute renal colic when diagnostic uncertainty is present during a patient encounter. Renal POCUS is not a technically difficult skillset to acquire, however, it is a unique skill that requires specific education and should not be clinically utilized prior to credentialing and/or approval which may be required depending upon one’s practice environment. Repetitious visualization of the kidneys on POCUS is helpful in learning how to distinguish between the presence and the absence of hydronephrosis. The urgent care clinician can adopt and incorporate renal POCUS into their practice to help low risk individuals avoid the emergency department while simultaneously reducing fragmentation of care, reduced radiation and increasing diagnostic accuracy at the bedside.
Citation: Burgin CM, Fredrick JW, Eicken J. A POCUS-based approach to acute renal colic in the urgent care center. J Urgent Care Med. October 2020. Available at: https://www.jucm.com/a-pocus-based-approach-to-acute-renal-colic-in-the-urgent-care-center/
REFERENCES
1. Westphalen AC, Hsia RY, Maselli JH, Wang R, Gonzales R. Radiological imaging of patients with suspected urinary tract stones: National trends, diagnoses, and predictors. Acad Emerg Med. 2011;18(7):699-707.
2. Moore CL, Carpenter CR, Heilbrun ME, et al. Imaging in Suspected Renal Colic: Systematic Review of the Literature and Multispecialty Consensus. Ann Emerg Med. 2019:1-9.
3. Coursey CA, Casalino DD, Remer EM, et al. ACR appropriateness criteria® acute onset flank pain-suspicion of stone disease. Ultrasound Q. 2012;28(3):227-233.
4. Riddell J, Case A, Wopat R, et al. Sensitivity of emergency bedside ultrasound to detect hydronephrosis in patients with computed tomography-proven stones. West J Emerg Med. 2014;15(1).
5. Leo MM, Langlois BK, Pare JR, et al. Ultrasound vs computed tomography for severity of hydronephrosis and its importance in renal colic. West J Emerg Med. 2017;18(4):559-568.
6. Mathews JD, Forsythe AV, Brady Z, et al. Cancer risk in 680 000 people exposed to computed tomography scans in childhood or adolescence: Data linkage study of 11 million Australians. BMJ. 2013;346(7910).
7. VII) NRC (US) C on HE of E to LL of IR (BEIR. Health Effects of Exposure to Low Levels of Ionizing Radiations. Washington, DC: National Academies Press; 1998.
8. Smith-Bindman R, Aubin C, Bailitz J, et al. Ultrasonography versus Computed Tomography for Suspected Nephrolithiasis. N Engl J Med. 2014;371(12):1100-1110.
9. Wong C, Teitge B, Ross M, et al. The accuracy and Prognostic value of point-of-care ultrasound for nephrolithiasis in the emergency department: a systematic review and meta-analysis. Acad Emerg Med. 2018;25(6):684-698.
10. Carbone A, Al Salhi Y, Tasca A, et al. Obesity and kidney stone disease: A systematic review. Minerva Urol e Nefrol. 2018;70(4):393-400.
11. Chen Z, Prosperi M, Bird VY. Prevalence of kidney stones in the USA: The National Health and Nutrition Evaluation Survey. J Clin Urol. 2019;12(4):296-302.
12. Renal and Urology News. Ultrasound Still Underused for Initial Imaging of Acute Renal Colic. Available at: https://www.renalandurologynews.com/home/conference-highlights/aua-2018-coverage/ultrasound-still-underused-for-initial-imaging-of-acute-renal-colic/. Accessed April 2, 2020.
13. Pathan SA, Mitra B, Mirza S, et al. Emergency physician interpretation of point-of-care ultrasound for identifying and grading of hydronephrosis in renal colic compared with consensus interpretation by emergency radiologists. Acad Emerg Med. 2018;25(10):1129-1137.
Author affiliations: Chelsea Burgin, MD, FAAFP, Prisma Health. James Fredrik W. Pike, MSIII, University of South Carolina School of Medicine. John Eicken, MD, EdM, Prisma Health.