Urgent message: The differential diagnosis of abdominal pain is challenging because many symptoms and signs are nonspecific and because patients might often have concomitant medical conditions that could cause abdominal pain. Although diverticulitis is more common in older patients, failure to consider diverticulitis in the differential diagnosis of abdominal pain in the younger adult could lead to delayed diagnosis and undesirable complications.
Fabrizia Faustinella, MD, PhD, FACP and L. Alexandre Frigini, MD
Introduction
Diverticular disease of the colon is a significant cause of hospitalization in industrialized societies and an important contributor to healthcare costs. Several lifestyle factors have been associated with diverticular disease, including low dietary fiber intake, high red meat intake, lack of physical activity, high BMI (≥25 Kg/m2), and smoking (≥40 pack-years).1 Diverticulitis usually presents with left lower quadrant pain, low-grade fever, nausea, and changes in bowel habits, but patients may also have right lower quadrant or suprapubic pain, associated with dysuria and urinary frequency.
The prevalence of diverticulosis increases with age, from <20% at age 40 to 60% at age 60. Approximately 5% to 15% percent of patients with diverticulosis develop acute diverticulitis.2,3 While the incidence of acute diverticulitis is higher in older individuals, approximately 16% of hospital admissions for acute diverticulitis are in patients under 45 years of age.4 Up to 50% of patients will experience recurrent bouts of diverticulitis.5 Although increasing age is associated with a higher risk of both local and systemic complication, the risk of recurrence seems to be higher in the younger individual.6
Presentation
A 38-year-old male presented to our walk-in clinic with a complaint of left lower abdominal pain, radiating to the left groin, for 3 days. The patient also reported abdominal bloating, nausea, reduced appetite, dysuria, urinary frequency, and chills. He denied hematochezia, diarrhea, and vomiting. The patient stated that he had experienced severe constipation in the past and, as he hadn’t had a bowel movement in over 4 days, he took laxatives at home; however, the abdominal pain did not improve. He also reported a history of kidney stones, but stated that the pain he experienced at that time felt “different” from the current episode.
On physical exam, the patient looked anxious and in mild distress. In addition, we found:
- BP 120/70
- HR 113
- Temp 100.3⁰ F
- RR 18
- SpO2 97%
- BMI 28.99
- Lungs: Clear to auscultation bilaterally
- Heart: Tachycardic, regular rhythm, no rub/gallop/murmur
- Abdomen: BS +; significant LLQ tenderness to palpation; + rebound tenderness; LLQ + rigidity
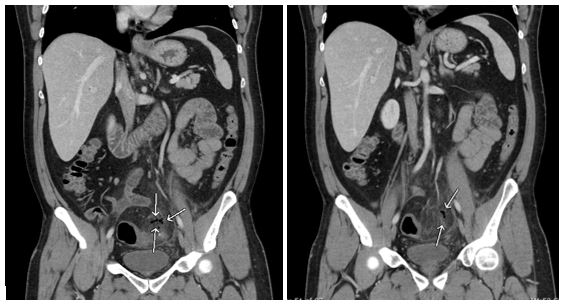
The patient was taken via wheelchair to the emergency department, located down the hallway from our clinic, due to the concern for an intra-abdominal disease process, abscess and/or perforation, with early signs of peritonitis, as indicated by the physical exam findings. In the ED, a CT of the abdomen and pelvis with IV contrast was immediately requested for further evaluation. The CT scan was read as:
- Gastrointestinal tract with hyperenhancement and focal colonic thickening of the sigmoid colon with adjacent pericolonic fat stranding and trace of free fluid.
- Sigmoid colon diverticulitis with extraluminal foci of air representing contained perforation.
Laboratory tests showed a WBC of 14.4 (ref. 4.5-12.0) with 75% neutrophils (ref. 34-67.9%).
The patient was admitted to the hospital and was medically managed with bowel rest, IV antibiotics (metronidazole and ciprofloxacin), and serial abdominal exams. He showed gradual improvement and was discharged, 4 days after admission, on oral antibiotics with a 3-week follow-up in the colorectal clinic and a 6-week follow-up for colonoscopy.
One month after discharge, the patient presented again to the ED with complaint of severe left lower quadrant pain x 1 day and was found to have perforated diverticulitis. The CT abdomen and pelvis was read as follows:
Interval evolution of contained perforated diverticulitis within the left lower quadrant. Interval worsening of pericolonic fat stranding and phlegmonous change without frank abscess formation. No significant t change in the amount of extraluminal air.
The patient was admitted to the surgery service where he was managed again conservatively with IV antibiotics and bowel rest. After 3 days of hospitalization, he was discharged home on oral antibiotics for a total of 14 days’ course.
A colonoscopy was performed 2 months after discharge and showed the presence of diverticulosis in the sigmoid colon and a pedunculated polyp, which was found to be benign.
Discussion
Diverticulitis, defined as inflammation of a diverticulum, is triggered by the erosion of the diverticular wall, caused by increased intraluminal pressure. This leads to inflammation and necrosis, with resulting micro or macro perforation of the diverticulum.
Lifestyle factors associated with diverticular disease described previously—low dietary fiber intake, high red meat intake, lack of physical activity, high BMI (≥25) and smoking (≥40 pack-years)1—applied to our patient.
Abdominal pain is the most common symptom in patients with acute diverticulitis. In the vast majority of cases, the pain is located in the left lower quadrant due to involvement of the sigmoid colon. However, patients may report suprapubic pain due to irritation of the bladder from the inflamed sigmoid colon7 and right lower quadrant pain due to more uncommon cecal diverticulitis. Our patient reported suprapubic pain associated with symptoms of dysuria and urinary frequency.
These symptoms, along with the previous history of kidney stones, could have been deceiving and could have led to the wrong clinical diagnosis. Changes in bowel habits are commonly associated with acute diverticulitis, with constipation affecting about 50% of patients and diarrhea 25% to 35% of patients.7
Our patient reported constipation, although that seemed to be a chronic issue for him, another confounding factor. Nausea and vomiting can develop due to ileus, caused by peritoneal irritation or bowel obstruction. Our patient reported nausea, no vomiting. On physical exam, patients may have localized peritoneal signs with guarding, rigidity, and rebound tenderness, which were all found in our case.
The vast majority of patients with acute diverticulitis have no associated complications.
Our patient’s CT scan showed focal colonic thickening of the sigmoid colon with adjacent pericolonic fat stranding and extraluminal foci of air representing contained perforation—common findings in acute uncomplicated diverticulitis. Computed tomography of the abdomen has very high sensitivity and specificity (94% and 99%, respectively) for the diagnosis of acute diverticulitis and can exclude other causes of abdominal pain.8 About 15% of patients with acute diverticulitis have an associated complication, such as an abscess, frank perforation (free air under the diaphragm), fistula formation, or colonic obstruction.9
Advanced age, male sex and several drugs, such as NSAIDs, opioids, and corticosteroids have been associated with an increased risk for perforation.10,11
Indications for inpatient treatment include:12
- CT showing complicated diverticulitis
- Acute uncomplicated diverticulitis associated with: high fever (≥102.5⁰ F), sepsis, micro perforation (a few air bubbles just outside the colon or confined to the pelvis), significant leukocytosis, severe abdominal pain and diffuse peritonitis, advanced age, comorbidities, intolerance of oral intake, noncompliance/lack of social support/difficult access to healthcare, and failed outpatient treatment.
Figure 1. CT coronal scan: free air (focal pneumoperitoneum).
Our patient was admitted to the hospital due to the presence of micro perforation, tachycardia, leukocytosis, fever, and signs of peritonitis (although localized). He was treated with IV ciprofloxacin and metronidazole, which provide coverage for the gastrointestinal flora of gram-negative rods and anaerobes, particularly Escherichia coli and Bacteroides fragilis.
Following conservative management of a first attack, approximately one-third of patients will have a second attack; this is exactly what happened to our patient 1 month after the first hospitalization. Overall, between 16% and 42% of patients have one or more recurrent attacks after nonoperative management.13,14
Although some studies have reported more severe recurrences of diverticulitis in patients younger than 40 years of age, other studies have not confirmed these findings.15,16
Overall, approximately 20% of patients with acute diverticulitis will require surgical intervention at a point in time, due to a complicated episode or multiple uncomplicated episodes of diverticulitis.
At around 6 weeks, after resolution of the symptoms of acute diverticulitis, patients should undergo a colonoscopy to rule out colon cancer and other underlying pathology. In our particular case, patient was found to have diverticulosis, as expected, and a benign colon polyp.
Citation: Faustinella F, Frigini LA. Abdominal pain in the younger adult: let’s not forget acute diverticulitis. J Urgent Care Med. July-August 2019. Available at: https://www.jucm.com/abdominal-pain-in-the-younger-adult-lets-not-forget-acute-diverticulitis/.
References
- Liu PH, Cao Y, Keeley BR, et al. Adherence to a healthy lifestyle is associated with a lower risk of diverticulitis among men. Am J Gastroenterol. 2017; 112(12):1868-1876.
- Parks TG. Natural history of diverticular disease of the colon. A review of 521 cases. Br Med J. 1969; 4(5684):639-642.
- Shahedi K, Fuller G, Bolus R, et al. Long-term risk of acute diverticulitis among patients with incidental diverticulosis found during colonoscopy. Clin Gastroenterol Hepatol. 2013;11(12):1609-1613.
- Nguyen GC, Sam J, Anand N. Epidemiological trends and geographic variation in hospital admissions for diverticulitis in the United States. World J Gastroenterol. 2011;17(12):1600-1605.
- Binda GA, Arezzo A, Serventi A, et al. Multicenter observational study of the natural history of left-sided acute diverticulitis. Br J Surg. 2012;99(2):276-285.
- Bharucha AE, Parthasarathy G, Ditah I, et al. Temporal Trends in the Incidence and Natural History of Diverticulitis: a Population-Based Study. Am J Gastroenterol. 2015;110(11):1589-1596.
- Textbook of Gastroenterology, Yamada T, Alpers DH, Kaplowitz N, et al (eds). Lippincott Williams & Wilkins, Philadelphia, PA; 2003.
- Lameris W, van Randen A, Bipat S, et al. Graded compression ultrasonography and computed tomography in acute colonic diverticulitis: meta-analysis of test accuracy. Eur Radiol. 2008;18(11):2498-2511.
- Onur MR, Akpinar E, Karaosmanoglu AD, et al. Diverticulitis: a comprehensive review with usual and usual complications. Insights Imaging. 2017;8(1):19–27.
- Morris CR, Harvey IM, Stebbings WSL, et al. Epidemiology of perforated colonic diverticular disease. Postgrad Med J. 2002;78(925):654-658.
- Böhm SK. Risk factors for diverticulosis, diverticulitis, diverticular perforation, and bleeding: a plea for more subtle history taking. Visceral Med. 2015;31(2):84-94.
- Feingold D, Steele SR, Lee S, et al. Practice parameters for the treatment of sigmoid diverticulitis. Dis Colon Rectum. 2014;57(3):284-294.
- Rose J, Parina RP, Faiz O, et al. Long-term outcomes after initial presentation of diverticulitis. Ann Surg. 2015;262(6):1046-1053.
- Binda GA, Arezzo A, Serventi A, at al. Multicenter observational study of the natural history of left-sided acute diverticulitis. Br J Surg. 201;99(2):276-285.
- Vignati PV, Welch JP, Cohen JL. Long-term management of diverticulitis in young patients. Dis Colon Rectum. 1995;38(6):627-629.
- Ritz JP, Lehmann KS, Stroux A, et al. Sigmoid diverticulitis in young patients—a more aggressive disease than in older patients? J Gastrointest Surg. 2011;15(4):667-674.
- Allan SB. Are antibiotics necessary in acute uncomplicated diverticulitis? NEJM Journal Watch. August 16, 2018. Available at: https://www.jwatch.org/na47292/2018/08/16/are-antibiotics-necessary-acute-uncomplicated. Accessed June 11, 2019.
- Peery AF. It’s actually a little complicated: antibiotics for uncomplicated diverticulitis. Am J Gastroenterol. 2018;113(7):949-950.
Fabrizia Faustinella, MD PhD FACP is Associate Professor of Medicine, Baylor College of Medicine, Houston TX. L. Alexandre Frigini, MD is Associate Professor of Diagnostic Radiology, Baylor College of Medicine, Houston, TX.
