Urgent message: Acute compartment syndrome (ACS) is an important high-risk diagnosis to exclude when evaluating peripheral extremity injury. Providers must maintain a high clinical index of suspicion with careful attention to the history and mechanics of injury in an urgent care setting to preclude the devastating, rapidly developing sequela of ACS. Missing a case of ACS may result in significant morbidity—and even mortality. Awareness of both subtle and overt signs will ensure the best care of the urgent care patient.
There are multiple case reports throughout the literature detailing the development of acute compartment syndrome (ACS) following thermal burns, crush injuries, bandages that are too tight, and several other mechanisms.1-6 The case below will serve as a framework for further discussion of compartment syndrome and how awareness of the mechanism of injury is critical to the evaluation of injuries that may precipitate ACS.
Case Presentation
A 15-year-old male presents to urgent care after running and jumping 4 feet into a shallow ravine and landing on a rock, twisting his right knee and ankle. Evaluation revealed pain in the lower right thigh, lateral aspect of the right knee and medial aspect of the right ankle, accompanied by decreased strength on plantar and dorsiflexion of the right leg compared with the left leg.
Examination of the right knee and ankle was notable for swelling, with no deformity or crepitus upon palpation. Neither joint demonstrated any gross instability, and the dorsalis pedis pulses and posterior tibial pulses were found to be equal bilaterally. X-ray images of the right femur, tibia/fibula, and foot were negative for fracture and dislocation. They were positive for an effusion in the right lateral knee. The patient was discharged home with an elastic bandage, acetaminophen, ibuprofen, range-of-motion activities, and follow-up instructions.
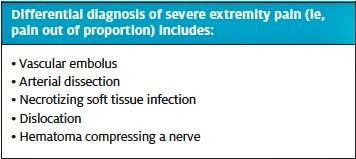
Three days later, the patient returned with worsening pain, nonresponsive to medication and accompanied by increased right lower leg swelling. On examination, the right lower leg was extremely tender to palpation (pain aggravated by flexion), swollen (right calf measured as 42 cm compared with the left calf measured as 33.5 cm), and cool to touch, with notable ecchymosis. The right dorsalis pedis pulse was noted as weak and difficult to palpate, and sensation was decreased. The differential diagnosis included deep vein thrombosis, swelling secondary to muscular strain, and ACS.
The patient was transported emergently to the hospital, where it was discovered that he had ACS complete to a popliteal artery transection. He underwent emergent surgery for anterior, lateral, and posterior compartment fasciotomy and repair of his popliteal artery.
Discussion
What is Acute Compartment Syndrome?
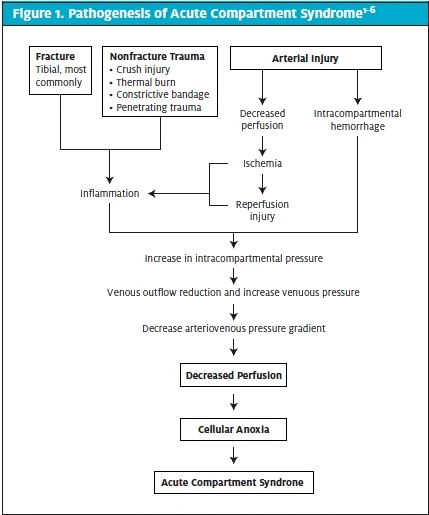
Acute compartment syndrome is a rapidly progressive neurovascular compromise and collapse within an anatomical compartment. The fascia that defines anatomic compartments is composed of dense fibrous connective tissue, unyielding to increased pressure. ACS occurs when intracompartment pressure increases and is a surgical emergency, as the risk of ischemia, necrosis, and permanent damage is high.
ACS can develop from a multitude of causes, all converging on a common pathogenesis of cellular anoxia leading to irreparable damage. Trauma most often precipitates the development of ACS, accounting for a vast majority of cases. One recent study by Marchesi found 63.6% of ACS cases to be due to trauma; a study by Hope showed 69% of ACS cases developed following fracture.7,8 Of traumatic causes, long-bone fracture is overwhelmingly the most common, accounting for 75% of cases.3,7,8
ACS has also been shown to develop secondary to elective procedures, especially involving ischemia reperfusion, and patients receiving anticoagulation therapy. Hope found that 10% of ACS cases associated with non-fracture injuries developed in patients who either had an underlying bleeding disorder or were receiving anticoagulation therapy.7,8 The reliable association between fracture injury and ACS development overshadows non‒trauma-related ACS cases, often resulting in a delay in diagnosis. Hope, specifically, found that ACS cases without fracture had a mean time to fasciotomy 12.4 hours longer than those cases occurring secondary to facture.8 ACS most commonly occurs in the lower extremity, and the most common preceding trauma is a posterior tibiofibular dislocation, with potential involvement of the popliteal artery.1,9-11
Locations of ACS
While the lower extremity is the most common site of ACS, other worrisome areas include the buttock, forearm, wrist, and hand.3,10 Both the wrist and hand share similar mechanisms of vascular compromise to the lower extremity. The buttock, however, has a more varied blood supply, with rich anastomosis. When ACS develops in this region, it is most commonly secondary to procedures; thus, the recognition and evaluation have a different course.7
Regardless of the site affected, the outcomes of ACS are dramatic, as the final common pathogenesis is cellular anoxia leading to irreparable damage. ACS cases almost always result in significant loss of function, and even limb amputation.9,10
Symptoms and Signs of Acute Compartment Syndrome
The pathogenesis of ACS is such that the extent of damage will not be apparent at initial presentation. While acute inflammation has a quick onset and is usually self-limited, associated edema does not reach a maximum until hours to days after an acute trauma. This delay puts many patients at risk of developing ACS. Those familiar with pathology recognize and anticipate the 5 Ps of ischemia: pulselessness, pallor, pain, paresthesia, and paralysis.3 Of these hallmark signs, pain is the only variable present in all cases of ACS. While pulselessness, pallor, paresthesia, and paralysis present as ACS progresses, they reflect a state of ischemia, suggesting that irreparable damage may already have occurred.
The most prevalent symptom of ACS is pain disproportionate to the injury, and pain that increases with passive stretching.3
Clear signs of vascular injury include diminished or absent pulses and pale, cool skin.2,3 Unfortunately, these unmistakable signs are not always initially present, complicating prompt diagnosis.
In the case of compartment syndrome of the lower leg, the initial findings are not necessarily helpful for identification or diagnosis.3,12-14 Specifically, detection and evaluation of abnormal peripheral pulses on physical examination of knee dislocation are not an adequate evaluation of circulatory stability.
A metaanalysis of 284 knee dislocations found abnormal pedal pulses had a sensitivity of 0.79 (95% confidence interval [CI], 0.64-0.89), a specificity of 0.91 (95% CI 0.78-0.96), a positive predictive value of 0.75 (95% CI, 0.61-0.83), and a negative predictive value of 0.93 (95% CI, 0.85-.96).12 These findings were neither sensitive nor specific enough to detect vascular injury.12 In the present case, dorsalis pedis and posterior tibial pulses remained palpable, despite significant injury to the popliteal artery. Similarly, several confirmed cases of ACS feature warm skin at the dorsum of the foot and/or palpable peripheral pulses, highlighting these findings as misrepresentations of vascular integrity.4,14-18 These conclusions verify that physical exam findings of dorsalis pedis or posterior tibial pulses are insufficient to lower index of suspicion for ACS. Furthermore, posterior tibiofibular dislocation may not cause overt transactions of the popliteal artery,5,18 instead initiating traction injury to the arterial intima and/or media. In this case, the vessel appears falsely intact, and initiates a prothrombotic environment within the popliteal fossa, increasing the risk of thrombus formation several hours or days later.4,11,18
Testing
Current radiology, urgent care, and emergency medicine guidelines3,12,19,20 suggest that when a patient arrives to an urgent care center or emergency room with the complaint of traumatic knee pain, they should be assessed with imaging in addition to physical exam. The imaging modality of choice for a suspected fracture is plain x-ray, while MRI is preferred for suspected ligature or meniscal tear.20 Unfortunately, neither x-ray nor MRI provides adequate visualization of the vascular system to help guide clinical decision-making, including transfer and referral decisions. Disposition needs to be based on mechanism and exam findings.
ACS most commonly develops in adolescent males and is most often associated with a tibial fracture and posterior tibiofibular dislocation. The growth plates in this population may still be prominent, and may obscure tibial plateau fractures.1,2,11,21 This clinical nuance is further support for maintaining a high index of suspicion of ACS throughout any workup of knee trauma with history congruent with ACS risk factors. Especially in an urgent care environment, when x-ray may be the only available imaging modality, it is important to proceed with caution when ruling out fracture to avoid potential cases of ACS.
Measurement of compartment pressures is performed by an orthopedist in a critical care setting, typically.
ACS Secondary to Popliteal Artery Injury
The popliteal artery, a continuation of the femoral artery, is the main blood supply to the lower leg, passing through the popliteal fossa before branching to form the anterior and posterior tibial arteries. The artery’s close proximity to the joint capsule, paired with the resting tension across the fossa, makes the popliteal artery vulnerable to injury, especially in posterior tibiofemoral joint dislocations and general fractures. During complete knee flexion, the popliteal artery can become compressed, with vascular stability provided by the genicular anastamosis.22 Our case involved an unusual cause of ACS: injury to the popliteal artery. Though this is a rare finding, it serves to demonstrate the mechanism of ACS (ie, decreased or absent blood supply causing tissues ischemia and necrosis with ensuing swelling), confirmed by the finding of increased compartment pressures.
Maintain a High Index of Suspicion—Indications for Transfer
Patients presenting to urgent care with complaint and exam findings consistent with a potential for ACS should, after a brief evaluation, be transferred to an ED with the capabilities to perform compartment pressures using a handheld manometer, simple needle manometer system, or wick/slit catheter technique. All yield similar results, though utility depends on accessibility of the equipment and, most importantly, a high index of suspicion for ACS.12,23-25
Medical‒Legal Pearls
- ACS is more common in young males due to their propensity for high-velocity activities and their strong fascial structure.
- A high index of suspicion must be maintained; patients who have a potential high-risk injury should be evaluated for ACS.
- Explicit instructions should accompany all injuries and conditions that can lead to ACS; patients should be instructed on what signs or symptoms should prompt a return for re-evaluation.
- Do not rely on the presence of dorsalis pedis or posterior tibial pulse to exclude ACS.
- Referral for additional testing is paramount if the patient has a high-risk injury or has signs or symptoms consistent with ACS
- One study showed that 32% of claims stemmed from a delayed diagnosis and 23% of claims were because of missed diagnosis.7
Management
Fasciotomy is the appropriate treatment of ACS. It should be performed emergently to relieve elevated compartment pressures and restore blood flow. If the extremity has already become necrotic, amputation may be necessary.
Conclusion
The take-home is that history and mechanics of the injury are essential clues in determining whether a patient is at risk for ACS. Cases of potential knee dislocation should always be approached with a high index of suspicion and thorough history guided, but not dictated, by a careful physical exam. Assessing joint stability by accurate anterior and posterior drawer test, as well as palpating distal pulses and assessing capillary refill, are necessary parts of the physical exam; however, normal findings are certainly not sufficient to rule out hemodynamic compromise that could potentially progress to ACS. “Pain out of proportion” is an important clue to look for a life- or limb-threatening cause of symptoms.
Citation: Shufeldt J, Nichta C. Acute compartment syndrome – an urgent care review. J Urgent Care Med. April 2017. Available at: https://www.jucm.com/acute-compartment-syndrome-urgent-care-review/.
References
- Pearse MF, Nanchahal J. Acute compartment syndrome: reducing the risk. Clinical Risk. 2008;14(3):114–118.
- Elliott KG, Johnstone AJ. Diagnosing acute compartment syndrome. J Bone Joint Surg Br. 2003;85(5):625-632.
- Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 6th ed. Philadelphia, PA: Mosby Inc; 2005.
- Downey-Carmona FJ, Gonzalez-Herranz P, De La Fuente-Gonzalez C, Castro M. Acute compartment syndrome of the foot caused by a hemangioma. J Foot Ankle Surg. 2006;45(1):52-55.
- Kim JW, Sung CM, Cho SH, Hwang SC. Vascular injury associated with blunt trauma without dislocation of the knee. Yonsei Med J. 2010;51(5):790-792.
- Olson SA, Glasgow RR. Acute compartment syndrome in lower extremity musculoskeletal trauma. J Am Acad Orthop Surg. 2005;13(7)436–444.
- Marchesi M, Marchesi A, Calori GM, et al. A sneaky surgical emergency: acute compartment syndrome. Retrospective analysis of 66 closed claims, medico-legal pitfalls and damages evaluation. 2014;45 Suppl 6:S16-S20.
- Hope MJ, McQueen MM. Acute compartment syndrome in the absence of fracture. J Orthop Trauma. 2004;18(4):220-224.
- Frink M, Hildebrand F, Krettek C, et al. Compartment syndrome of lower leg and foot. Clinical Orthop Relat Res. 2010;468(4):940–950.
- Matsen FA, Veith RG. Compartmental syndromes in children. J Pediatric Orthop. 1981;1(1):33–41.
- Shore BJ, Glotzbecker MP, Zurakowski D, et al. Acute compartment syndrome in children and teenagers with tibial shaft fractures. J Orthop Trauma. 2013;27(11):616-621.
- Speer M, Shufeldt J. Chronic exertional compartment syndrome. J Urgent Care Med. 2013;7(6):22-26.
- Barnes CJ, Pietrobon R, Higgins LD. Does the pulse examination in patients with traumatic knee dislocation predict a surgical arterial injury? A meta-analysis. J Trauma. 2002;53(6):1109-1114.
- Ulmer T. The clinical diagnosis of compartment syndrome of the lower leg: are clinical findings predictive of the disorder? J Orthop Trauma. 16(8):572–577.
- Johnson MW. Acute knee effusions: a systematic approach to diagnosis. Am Fam Physician. 2000;61(8):2391-2400.
- Henning A, Gaines RJ, Carr D, Lambert E. Acute compartment syndrome of the foot following fixation of a pilon variant ankle fracture. Orthopedics. 2010;33(12):926.
- Klovning J, Beadle T. Compartment syndrome secondary to spontaneous rupture of a Baker’s cyst. Journal La State Med Soc. 2007;159(1):43-44.
- Godinger JJ, de Bat JM, Lecestre P, et al. [Compartment syndrome of the Leg (author’s transl)]. Rev Chir Orthop Reparatrice Appar Mot.1979;65(4):221-229.
- Resnick L, Shufeldt J, eds. Textbook of Urgent Care Medicine. Scottsdale, AZ; Urgent Care Textbooks; 2013.
- Uliasz A, Ishida JT, Fleming JK, Yamamoto LG. Comparing the methods of measuring compartment pressures in acute compartment syndrome. Am J Emerg Med. 2003;21(2):143-145.
- Referring physician ordering guide: What to order when. Available at: http://www.radiax.com/Portals/1/Documents/Downloadable%20Materials/General%20Radia/RadiaImCtrs_OrderingGuideF_Jun12.pdf2012.
- Moore KL, Dalley AF, Agur AMR, eds. Moore Clinically Oriented Anatomy. 7th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins Health, 2013.
- McDermott MM, Criqui MH, Liu K, et al. Lower ankle/brachial index, as calculated by averaging the dorsalis pedis and posterior tibial arterial pressures, and association with leg functioning in peripheral arterial disease. J Vasc Surg. 2000;32(6):1164–1171.
- Whitesides TE, Haney TC, Morimoto K, Harada H. Tissue pressure measurements as a determinant for the need of fasciotomy. Clin Orthop Relat Res. 1975;113:43-51.
- Barnes MR, Gibson MJ, Scott J, et al. A technique for the long term measurement of intra-compartmental pressure in the lower leg. J Biomed Eng. 1985;7(1):35-39.
John Shufeldt, MD, MBA, JD, FACEP and Carli Nichta MS-3

John Shufeldt, MD, JD, MBA, FACEP
