Urgent message: Summer brings increased participation in outdoor activities and sports in which patients are likely to sustain injury. Patients with thigh injuries, such as injury to the quadriceps and patellar tendon, may present to the urgent care center. Timely diagnosis is essential in preserving strength and function of the quadriceps complex.
TRACEY QUAIL DAVIDOFF, MD
Patients who run and jump are at risk for injuring their quadriceps complex. These activities are common in the summertime. Although the majority of these injuries are simple strains, more severe injury to the quadriceps complex can occur, resulting in severe pain, loss of function, and permanent weakness of the thigh. The urgent care provider needs to be astute in diagnosing these injuries by taking a thorough medical history, focusing on the specific mechanisms of injury. This should be followed by a comprehensive musculoskeletal examination focusing on the injured extremity. Providers should keep in mind which patients will benefit from early referral to the hospital or orthopedic surgeon. Severe injuries may require surgical repair. Understanding the anatomic relationships and mechanisms of injury is key to determining the correct diagnosis and course of treatment.
Case Presentation
A 30-year-old man presented to the urgent care center after injuring his leg while playing kickball. The patient stated that he was nearing second base when he stopped briefly and then decided to turn and run to third base. Upon pivoting on his left leg with his foot planted, he felt a pop in his left knee, followed by severe pain in the thigh that made him collapse. He reported feeling as though his knee was dislocated. He was unable to straighten the knee fully, and continued to have severe pain. He had no previous injuries to the left knee and no other injuries from this incident.
The patient, a chef, had no significant past medical history except for dislocation of his other kneecap when he was a high school student. He reported that he takes no medication and does not smoke or take street drugs, and that he drinks alcohol socially.
Observations and Findings
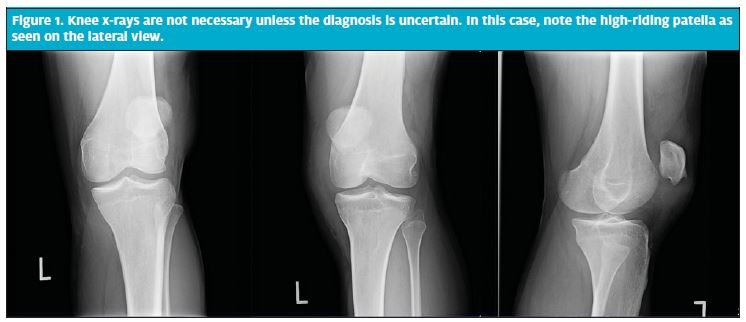
On examination, the patient was clearly uncomfortable. He was sitting in a wheelchair, holding his left leg with both the hip and the knee flexed at about 45°.This position caused him the least pain. There was no redness or bruising of the thigh. There was an obvious knee effusion. The patella was proximally displaced. The patient had no bony tenderness at the knee, hip, femur, tibia, or fibula. In comparison with the uninjured right thigh, the left thigh had an obvious defect in the distal quadriceps. The proximal quadriceps had swelling and tenderness. Any attempts to get the patient to extend the hip or knee were met with resistance because of pain. Pulses and sensation in the left foot were normal. The patient was unable to weight bear because he was unable to straighten his left leg. Radiographs of the patient’s knee showed no fracture or dislocation but did show a high-riding patella (Figure 1).
Diagnosis and Disposition
The diagnosis was rupture of the quadriceps. The patient was given ketorolac and fentanyl for pain, which provided some pain relief. He refused an ambulance because of its cost, so he was fitted with crutches and his leg was wrapped with an elastic bandage and knee immobilizer. His girlfriend drove him to a local emergency department for definitive care.
Discussion
Anatomy
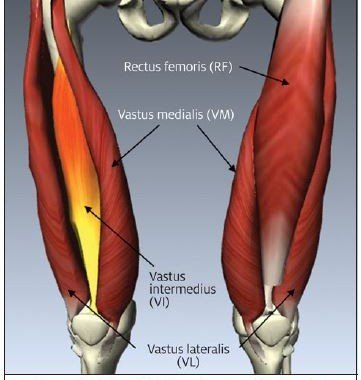
The quadriceps are a group of 4 muscles in the anterior thigh: the rectus femoris, vastus lateralis, vastus medialis, and the vastus intermedius (Figure 2). These muscles function together to allow knee extension, hip flexion, pelvic stabilization, and control of deceleration and landing when a person is running and jumping. Strains and ruptures of the quadriceps complex are common in athletes in such sports as basketball, volleyball, soccer, and football.1
Clinical Presentation
Strains of the quadriceps occur during movements involving sudden, forceful contractions, and they cause pain and dysfunction that may occur immediately or even several days after injury.2 Depending upon the extent of injury, pain may be mild, moderate, or severe. Pain usually increases with passive or active flexion or extension of the knee. In severe cases, there may be significant swelling and ecchymosis. Anterior thigh pain will be present with weight bearing.
Quadriceps and patellar tears and complete ruptures are relatively uncommon.3 Rupture more commonly occurs distal to the patella than proximal to it. Rupture occurs after a sudden, strong contraction of the quadriceps muscle, as when landing from a jump or making a sudden change in direction at high speed. There will be a severe, sharp pain at the knee that may be immediately disabling. This may also occur when a patient falls backward, bending at the knee with their feet in a fixed position. Quadriceps tendon ruptures are more common in patients older than 40 years, and patellar tendon ruptures are more common in patients younger than 40 years.
The patient will be obviously uncomfortable and will prefer to hold both the hip and knee in flexion. There may or may not be an obvious defect in the distal anterior thigh, with proximal swelling and bruising. In the injured leg, the patella may be proximally or distally displaced in comparison with the uninjured leg. Knee extension will be limited in partial tears, and impossible in complete tears. Patients with complete tears cannot initiate or maintain straight-leg-raising against gravity when supine.
Imaging
Diagnostic imaging is not required in quadriceps injuries1 because the diagnosis is usually readily made clinically. Radiographs may exclude patellar fracture or show displacement of the patella proximally or distally. Ultrasonographers experienced in musculoskeletal ultrasound may be able to quantify the degree of tear and confirm the diagnosis, but this is not required.
Treatment
Patients with complete tears and high-grade partial injuries should be referred for prompt surgical repair,4 usually within 7 to 10 days. Patients with injuries that are accompanied by massive bruising or hematoma formation are at risk for compartment syndrome and should be referred for immediate evaluation. Most partial tears are treated conservatively with ice, compressive dressings, pain medication, and gradual ambulation with crutches. Physical therapy should be provided after initial healing. Major complications are uncommon but can occur and include myositis ossificans, compartment syndrome, and chronic weakness. Improper treatment may result in the inability to return to full athletic activities.
Take-Home Points
The quadriceps muscle group is subject to injury during activities involving jumping and running. The majority of injuries are strains that can be handled with rest, ice, compression, and crutches. More serious injuries require orthopedic surgical repair in a timely manner to prevent the long-term complications of weakness and the inability to return to full sports activities.
References
- Golaspy JN, Steele MT. Knee injuries. In: Tintinalli JE, Stapczynski JS, Cline DM, et al, eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw-Hill Medical; 2010:1856–1864.
- Simon RR, Koenigsknecht SJ. Injuries to the thigh. In: Simon RR, Koenigsknecht SJ, eds. Emergency Orthopedics: The Extremities. 3rd ed. East Norwalk, CT: Appleton & Lange; 1996:428–430.
- Langer PR, Selesnick FH. Proximal rectus femoris avulsion in an elite, Olympic-level sprinter. Am J Orthop (Belle Mead NJ). 2010:39:543–547.
- Ilan DI, Tejwani N, Keschner M, et al. Quadriceps tendon rupture. J Am Acad Orthop Surg. 2003;11:192–200.
