Published on
Urgent message: Fever in pediatric patients, while frequent, is rarely the result of a serious illness. Urgent care practitioners must be able to consistently distinguish between serious and benign causes with a minimum of invasive testing.
BRENDAN KILBANE, MD, FAAP
Introduction
Ever is one of the most common chief complaints in pediatric patients who present for urgent evaluation. A surprising number of families continue to suffer from “fever phobia,” with one study noting that 91% of parents believe that a fever alone could hurt their child.1 In the vast majority of pediatric patients who present with a fever, either physical exam will lead to identification of the source or the cause will be a self-limited viral illness. In a small percentage of children, however, the source of fever is a serious bacterial illness (SBI) such as a urinary tract infection (UTI), pneumonia, bacteremia, or meningitis. The challenge for an urgent care provider is to identify the patient who is at high risk of these SBIs with the least amount of invasive testing.
Background
Over the last 30+ years, the question of how best to manage the febrile pediatric patient has been the subject of countless studies. This research has primarily resulted in a variety of guidelines that identify groups of patients who are either at high or low risk of certain infections. That classification allows clinicians to decide if a patient requires treatment or admission. The other main finding of these studies is that different age groups have different risks of SBIs.2 As a result, it is helpful to group patients by age ranges when discussing what evaluation is required When evaluating a febrile pediatric patient, an urgent care provider’s first and most important task is determining whether the patient is “well or not well.” A good deal of research has been done in an attempt to quantify what exactly a clinician relies on to make this distinction, with limited success, and it appears that experienced urgent care providers should trust their clinical intuition because they are very good at recognizing well patients in the older age ranges. They should be more cautious, how- ever, when making this determination in younger patients or if they have limited exposure to pediatric patients on a regular basis.3,4
If a clinician determines that a patient is “not well,” then the child needs appropriate laboratory studies, treatment with antibiotics and transfer to a higher level of care, independent of the lab results or the patient’s age. If a patient is determined to be “well,” than an urgent care provider can use the following age-based approach to guide decision-making about additional laboratory evaluation and treatment.
Aged 0 to 28 Days
History and Physical
Fever in this age group is defined as a rectal temperature ≥38°C and a reading should be obtained along with a full set of vital signs on every patient. In this age group, the history of present illness is often brief and should focus on the family’s reporting of the infant’s level of arousal as well as his or her ability to feed.
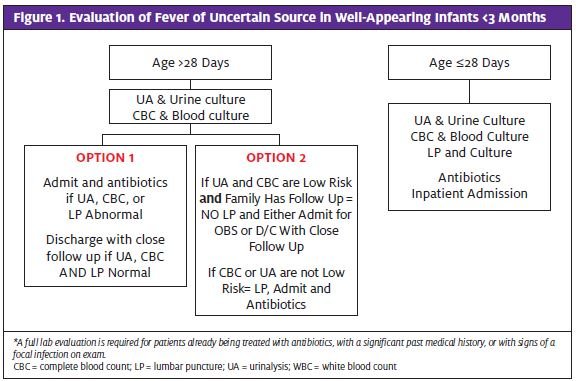
Past medical history should include details surrounding the infant’s delivery as well as a maternal history, including Group B streptococcus status. During the physical exam, an urgent care provider should pay particular attention to an infant’s general tone and appearance. Does the child arouse easily to stimulation? Is her or she irritable or unable to be consoled? Limp or flaccid? Given the difficulty in localizing symptoms such as pain during an infant exam, it is recommend ed that even those who appear “well” be managed aggressively (Figure 1).
Evaluation and Management
Numerous studies have documented a high rate of SBI—approximately 10% to 20%—in febrile infants.5 Based on this high risk, the American College of Emergency Physicians and the American Academy of Pediatrics currently recommend that these infants receive a “full septic work up.” Such a work up includes a complete blood count (CBC) with blood culture, urinalysis (UA) obtained by catheterization or suprapubic aspiration with urine culture, lumbar puncture (LP) with cerebrospinal fluid (CSF) analysis and culture, and a chest x- ray (CXR) if the patient has any focal lung findings or hypoxia.2,6 All infants in this age group should be treated with antibiotics and admitted for observation. Initial intravenous (IV) antibiotics of choice include ampicillin 50 mg/kg and either gentamycin 3 mg/kg or cefotaxime 50 mg/kg.
Aged 28 to 90 Days
History and Physical
Fever continues to be defined as 38°C for this age range and a reading should be obtained rectally, along with a full set of vital signs. As with younger infants, the history should focus on the family’s impression of the infant’s general appearance, including any excessive sleepiness or irritability, and ability to feed. During the
physical exam, the urgent care provider should again observe the infant’s general tone and level of arousal. Many clinicians, depending on their experience, will be able to make a general impression as to whether the infant is “well or not well.” However, additional laboratory evaluation is required for even “well”-appearing infants in this age group. Any infant that a clinician feels is “not well” should have a full evaluation and be admit- ted for observation, independent of any laboratory results (Figure 1).
Evaluation and Management
Previous research has established that 5% to 10% of infants in this age group will have an SBI, the majority of which are UTIs, whereas 1.5% to 2% will be found to be bacteremic and 0.5% will have meningitis.7 An urgent care provider’s goal should be to classify each patient as either at high or low risk of having an SBI, which will then dictate if inpatient admission is required or management can safely be done on an outpatient basis.8 The process of classifying such patients by incorporating lab- oratory results into assessment arises from research from the 1990s that led to development of “city”-based criteria for Rochester, Boston, and Philadelphia, among others. Unfortunately, these criteria all use slightly different ages and lab values, which results in some minor variations among the recommendations.9-11
A reasonable approach is that ALL patients should receive a CBC with blood culture and a UA with urine culture obtained by catheterization. Patients with focal respiratory findings or hypoxia should have a CXR. A Patient is considered at low risk of SBI if he or she has the follow- ing results: A CBC with 5,000 to 15,000 WBCs and less than 1,500 bands, a UA with less than 10 WBCs/high-powered field and no bacteria on gram stain, and a CXR with no focal infiltrate concerning for pneumonia. This approach is supported by a clinical policy statement from ACEP and an expert panel of pediatric emergency medicine physicians, as well as evidence-based guidelines employed at a leading children’s hospital.2,6,12
The question is often raised about whether a less invasive approach would also be reasonable. Currently, however, there are minimal prospective data to support this approach. In one study of outcomes in febrile infants managed by general pediatricians, a non-guide- line-based approach was found to be equally effective, when judged by incidence of serious infections that were missed.13 However, 95% of the infants in that study had more than one encounter with their pediatrician. Because most urgent care providers cannot guarantee such close follow up, it is difficult to generalize these results to an acute care setting. This lack of continuity is a main driver behind the recommendations for such an aggressive approach to identify at-risk patients during an the initial patient encounter.
Another contested point when managing patients in this age range surrounds the need to perform a LP to rule out meningitis in a patient with a low-risk CBC and UA. More conservative sources advocate the necessity for LP to truly consider an infant low risk and that urgent care providers should err on the side of caution and perform an LP on all these patients because they may have inconsistent follow up. To support this position, they cite the fact that an LP is part of the Boston and Philadelphia criteria 9,11 and that a later study documented that up to 40% of all febrile infants, both well and not well, aged less than 90 days who were eventually diagnosed with a SBI had a CBC that would have made them low risk.14
Others argue that risk of meningitis is very small in infants aged 28 to 90 days and the vast majority of such patients are either “not well” or would have a CBC or UA that would classify them as high risk. To support this position, they cite that the Rochester criteria did not automatically include a LP for all such patients and they were able to accurately classify patients as high or low risk.10
Whether LP is required in all infants aged 28 to 90 days to classify them as low risk remains debated. How- ever, LP should be strongly considered in any patient with symptoms of systemic illness as well as in infants with a history of current antibiotic therapy, who have unreliable follow up or a complex medical history or who are being treated with IV antibiotics for any reason. Infants classified as high risk based on CBC or UA results should undergo LP before receiving antibiotics and should be admitted for a period of observation. Low-risk infants by lab results are eligible for outpatient observation but an urgent care provider must be confident that they are well-appearing and that the family has established follow up and can be contacted and will return promptly for treatment. If a clinician is not confident about these factors, such patients should be admitted for observation. Several studies support not treating low-risk patients with antibiotics before dis- charge, however, it is also acceptable to administer a single dose of ceftriaxone 50 mg/kg IV or intramuscularly.
Aged 3 to 36 Months
Background
The focus when evaluating patients with fever in this age group shifts from the approach used in younger infants, where a high risk of SBI requires a laboratory evaluation, to one where the goal is to use selective testing to identify the very small percentage that have an occult infection that may progress into a SBI.
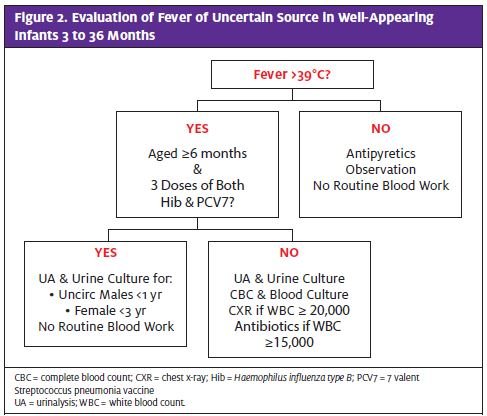
Research in the 1980s demonstrated that 2% to3% of well-appearing children with a temperature 39°C had bacteria in their bloodstream.15 It also found that of these patients, up to 20% would return days later with a serious illness including osteomyelitis, sepsis, or meningitis. Thus the practice of performing a “screening” CBC, UA, and cultures was introduced as a means of identifying these at-risk children before they returned with a focal infection. However, more recent data have raised the question of whether performing such screens—especially the CBC and blood culture—is still the right approach (Figure 2).
History and Physical Exam
In this age range, the height of fever that triggers further evaluation increases to 39°C. That does not mean that a child with a fever of 38.5°C cannot have an occult infection but, rather, that the risk is low enough to justify out patient observation without automatically obtaining lab- oratory data. It is again crucial to identify the patient as “well or not well.” If an urgent care provider judges a child to be “not well” based on the results of clinical exam, then aggressive evaluation, treatment with antibiotics, and transfer to a high level of care is required. Only a “well” child is a candidate for selective laboratory evaluation and antibiotic therapy.
Fortunately, arriving at this clinical assessment is easier because as patients age, they are able to provide a more useful history and physical, including information on focal signs and symptoms. It is still important to continue to involve the parents as they can relate any change in a child’s normal behavior that can serve as a possible clue for a localized process, such as not using an arm as a sign of a soft-tissue infection. In addition, particular attention should be paid to a patient’s immunization status, because advances in vaccinations have made a tremendous impact on each individual’s risk. Finally, vital signs become a more sensitive marker of occult illness and it becomes even more crucial to be aware of tachypnea and tachycardia, especially if it does not improve after administration of antipyretics.
Occult Bacteremia
As previously mentioned, the “screening” CBC and blood culture were introduced in the 1980s in an attempt to identify children whose fever was the only sign of bactermia (ie occult bacteremia) who were at risk of developing a localized infection. However, ongoing improvements in childhood vaccinations have resulted in a re-examination of this approach.
The Haemophilus influenza type b (Hib) vaccine was introduced in the late 1980s and has effectively eliminated Hib as a childhood pathogen in immunized patients. The 7-valent conjugate pneumococcal vaccine against Streptococcus pneumoniae (PCV7), introduced in 2000, also has had a dramatic impact. Initial surveillance has documented a decrease in Sp pneumoniae bacteremia by 70% to 90%.16 In addition, a 13-valent S pneumoniae vaccine was introduced in 2010 and is anticipated to result in an even larger decrease. Also of note is that surveillance data demonstrate that most children are actually receiving the immunizations. One study found that 85% to 90% of 3-year-olds had received at least 3 doses of PCV7.17 Finally, an impressive herd immunity has been demonstrated in patients who may not have received the vaccines so that their risk of invasive pneu- mococcal disease is decreasing as well.
As a result of these two vaccines, the risk of occult bacteremia in an immunized febrile patient is now approximately 0.2% to 0.5%, down significantly from the earlier rate of 2% to 3%.18 The clinical impact of these advances is that most guidelines are recommending that fewer patients have labs done as a screen for occult bacteremia.
A reasonable approach is to continue to perform a CBC and blood culture on “well”-appearing pediatric patients with a fever 39°C who have not yet received three Hib and three S pneumoniae vaccinations. If the family is unsure if all three vaccinations have been given, it is reasonable to proceed as if they have not been given. Because these vaccines are currently recommended to be given at ages 2, 4, and 6 months, most patients older than age 6 months will not require blood work as part of their evaluation. The CBC results are currently still used to guide subsequent antibiotic therapy, with a WBC >15,000 or <5,000 indicating a slight increased risk of bacteremia. As a result, these patients should receive a dose of 50 mg/kg ceftriaxone IV/IM while their blood cultures are followed. Research is ongoing but to date there is no clear role for using other inflammatory markers specifically C-reactive protein or procalcitonin in place of the CBC as a screen for occult bacteremia.
Occult UTI
Although occult UTIs often receive significantly less attention than occult bacteremia, the numbers support that their diagnosis should actually be a higher priority for urgent care providers. Numerous studies have doc-umented approximately a 2% to 5% rate of UTI in well- appearing children with fever 39°C.19 This rate is concerning because most of these patients cannot give historical factors, such as dysuria, which would assist a clinician in reaching the diagnosis. However, research has identified other factors that can mark a patient as high risk and requiring additional testing.
The most important risk factor is patient gender because the prevalence of UTIs in females is more than twice that in males. In females, the two risk factors to consider are race and age. Several studies noted up to twice the risk of UTI in white females compared with non-white females. Younger female infants are at higher risk due to the fact that anatomical abnormalities, which predispose patients to UTIs, typically present by age 3 to 6 months. For males, the two factors to consider are age and circumcision status. Several studies have documented a risk of UTI 8 to 10 times higher in uncircumcised males than in circumcised males.20,21 Younger males have a higher risk, again due to the role of anatomic abnormalities. Lastly, several studies document that having either a positive test for a viral illness (influenza and respiratory syncytial virus) or a clinical syndrome matching a viral illness decreased the risk of UTI by about half.22 Based on current recommendations, UA and urine culture are a reasonable approach to infants aged 3 to 6 months with a temperature 39°C who have no viral symptoms or whose fever has lasted longer than 2 days. For uncircumcised males, this recommendation holds true up to age 12 months. For females, this recommendation holds true until they are no longer using diapers and are able to indicate more specific symptoms by history.23 Obtaining a catheterized urine for culture is recommended for all patients until they are able to provide a voided specimen. Use of urine bags to obtain urine for culture is unreliable because they are associated with a very high rate of contamination. Some sources advocate use of a bag for screening UA in infants older than age 6 months, followed by culture by catheterization if the UA is positive for either nitrates or leukocytes. This is not recommended for younger infants because of the concern about false-negative UA results.19 Cultures should be obtained on any pediatric patient diagnosed with a UTI to confirm the diagnosis, which is critical to informing the decision for further outpatient evaluation, as well as to monitor for resistant pathogens.
The decision about treating these patients as outpatients versus inpatients should be made in concert with the family and their regular physician. Any patient with symptoms of a systemic illness, especially vomiting, requires inpatient treatment. Strong consideration also should be given to admission for infants aged 3 to 6 months because they are at slightly higher risk of concurrent bacteremia and less able to demonstrate that they do not have signs of systemic illness.
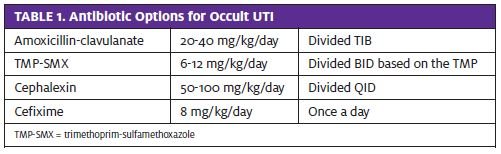
Ceftriaxone (75 mg/kg) is the recommended choice for either an initial dose before outpatient therapy or before transfer for inpatient admission. Oral therapy for 7 to 14 days should be guided by local resistance pat- terns for common urinary pathogens. Several reason- able options are listed in Table 1. Amoxicillin should be used cautiously because rates of resistance to common pathogens of up to 50% have been reported in some locations. As always, “not well”-appearing patients, especially those aged <1 year, will likely need transfer for a high level of care.
Occult Pneumonia
Concern for this entity arose from several studies that examined young febrile infants and included a screening CXR. The reports demonstrated signs of pneumonia on CXR in a small percentage of subjects who had no respiratory symptoms. Since that time, occult pneumonia remains a hotly debated topic with studies finding different rates, mainly depending on the type of patients enrolled, how a lack of respiratory symptoms was defined, and what constituted a positive finding on CXR. Current recommendations indicate that routine screening CXR is not required in patients aged 3 to 36 months with fever alone. CXR should be considered in patients with unexplained tachypnea, hypoxia, focal physical exam findings or whose fever has lasted longer than would be expected with a typical viral infection. CXR should also be considered in patients with a WBC > 20,000 without a source of infection on exam.24 Infants aged 3 to 6 mouths in whom pneumonia is diagnosed are likely to benefit from hospitalization. In addition, children with respiratory distress or oxygen saturation below 90% should be admitted for observation and IV antibiotics. For outpatient therapy, high-dose amoxicillin (80-100 mg/kg/day divided BID) for 10 days is recommended as first-line therapy. Azithromycin for atypical pneumonia is not routinely recommended in this age group unless indicated by the history or physical.25
References
- Crocetti M, Moghbeli N, Serwint . Fever phobia revisited: have parental misconceptions about fever changed in 20 years? Pediatrics. 2001;107(6):1241–1246.
- American College of Emergency Physicians Clinical Policies Committee: Clinical policy for children younger than three years presenting to the emergency department with Annals Emerg Med. 2003;42(4):530-545.
- McCarthy PL, Lembo RM, Fink HD, et Observation, history, and physical examination in diagnosis of serious illnesses in febrile children less than or equal to 24 months. J Pedi- atr. 1987;Jan; 110(1):26-30.
- Baker MD, Avner JR, Bell Failure of Infant Observation Scales in Detecting Serious Illness in Febrile, 4-to 8-Week-Old Infants. Pediatrics. 1990; 85: 1040-1043.
- Baker MD, Bell L M. Unpredictability of serious bacterial illness in febrile infants from birth to 1 month of Arch Pediatr Adolesc Med. 1999;153:508–511.
- Baraff Baraff LJ, Schriger DL, Bass Practice Guideline for the Management of Infants and Children 0 to 36 Months of Age With Fever Without Source Pediatrics. 1993;92;(1):1-12.
- Byington CL, Enriquez FR, Hoff C, et Serious Bacterial Infections in Febrile Infants 1 to 90 Days Old With and Without Viral Infections. Pediatrics. 2004;113(6): 1662 -1666.
- Ishimine, Fever without source in children 0 to 36 months of age. Ped Clin North Am. 2006;53(2):167-194.
- Baker MD,Bell LM, Avner Outpatient management without antibiotics of fever in selected infants. N Engl J Med. 1993;329:1437.
- Jaskiewicz JA, McCarthy CA, Richardson AC, et Febrile infants at low risk for serious bacterial infection: an appraisal of the Rochester criteria and implications for management. Pediatrics. 1994;94:390–396.
- Baskin MN, O’Rourke EJ, Fleisher GR: Outpatient treatment of febrile infants 28 to 89 days of age with intramuscular administration of J Pediatr. 1992;120:22-27.
- FUS Team, Cincinnati Children’s Hospital Medical Center: Evidence-based clinical care guideline for fever of uncertain source in infants 60 days of age or less, http://www.cincin-org/svc/alpha/h/health-policy/ev-based/default.htm, Guideline 02, pages 1- 14, October 2010.
- Pantell RH, Newman TB, Bernzweig J, et Management and outcomes of care of fever in early infancy. JAMA. 2004;291:1203-1212.
- Bonsu BK, Harper Utility of the peripheral blood white blood cell count for identi- fying sick young infants who need lumbar puncture. Ann Emerg Med. 2003;41:206–214.
- Alpern ER, Alessandrini EA, Bell LM, et Occult bacteremia from a pediatric emergency department: Current prevalence, time to detection and outcome. Pediatrics. 2000;106:505- 511.
- Whitney CG, Farley MM, Hadler J, et Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N Engl J Med. 2003;348(18):1737-1746.
- Jacobs MR, Good CE, Bajaksouzian S, et Emergence of Streptococcus pneumoniae sero- types 19A, 6C, and 22F and serogroup 15 in Cleveland, Ohio, in relation to introduction of the protein-conjugated pneumococcal vaccine. Clin Infect Dis. 2008;47(11):1388-1395.
- Herz AM, Greenhow TL, Alcantara J, et Changing epidemiology of outpatient bac- teremia in 3- to 36-month-old children after the introduction of the heptavalent-conjugated pneumococcal vaccine. Pediatr Infect Dis J. 2006;25(4):293-300.
- American Academy of Pediatrics, Committee on Quality Improvement, Subcommittee on Urinary Tract Urinary tract infection: clinical practice guideline for the diagno- sis and management of initial urinary tract infections in febrile infants and children 2 to 24 months of age. Pediatrics. 2011;128(3):595–610.
- Shaw KN, Gorelick M, McGowan KL, et Prevalence of urinary tract infection in febrile young children in the emergency department. Pediatrics. 1998;102:1-5.
- Zorc JJ, Levine DA, Platt SL, et Clinical and demographic factors associated with uri- nary tract infection in young febrile infants. Pediatrics. 2005;116(3):644.
- Levine DA, Platt SL, Dayan PS, et Risk of serious bacterial infection in young febrile infants with respiratory syncytial virus infections. Pediatrics. 2004;113(6):1728-1734.
- 23,- Gorelick MH, Hoberman A, Kearney D, et al. Validation of Decision Rule Identifying Febrile Young Girls at High Risk for Urinary Tract Infections. Peds Emer Care. 2003;19(3):162:164.
- Bachur R, Perry H, Harper M, Occult pneumonias: Empiric chest radiographs in febrile children with Ann Emerg Med. 1999;33:166-173.
- Bradley JS, Byington CL, Shah SS, et The management of community-acquired pneu- monia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53:e25–76.