Urgent message: Obesity continues to be a significant health problem in the United States, with more and more patients opting for a surgical solution to their own weight loss challenges. As this trend continues, urgent care providers can expect to see more patients with post bariatric surgery complaints, ranging from the typical and benign to pulmonary emboli, anastomotic leaks, and respiratory failure account.
Tracey Quail Davidoff, MD, FCUCM
Obesity has become one of the foremost public health concerns in our time. It may result in poor self-esteem, depression, discrimination, as well as diabetes (DM), coronary artery disease (CAD), and obstructive sleep apnea (OSA). Because dieting in the morbidly obese is often futile or produces results that are short-lived, both providers and patients are looking for effective long-term solutions to this problem.
Bariatric surgery leads to sustainable long-term weight loss and may be curative for obesity-related conditions including DM and OSA.1 As the number of patients undergoing these procedures increases, the urgent care provider needs to be aware of early and late complications. Recognizing the serious complications, knowing how to treat, and what to refer are key in providing appropriate urgent care to these patients.
INTRODUCTION
In 2016, the CDC National Center for Health Statistics reported that 71% of U.S. adults over 20 were overweight, with 38% considered obese; this includes 21% of adolescents (12–19 years of age) and 17% of children (6–11 years of age).2 Obesity and its related complications are the leading cause of death in both the US and worldwide, with the resultant healthcare costs estimated to be $147 billion per year.2
Bariatric surgery may offer a long-term solution to those with morbid obesity. However, the postsurgery period is a lifelong commitment with permanent health and lifestyle changes that require strict compliance.3
INDICATIONS FOR BARIATRIC SURGERY
Indications for bariatric surgery include a BMI of >40 or a BMI of >35 with obesity-related comorbidities such as DM, OSA, CAD, nonalcoholic fatty liver, refractory hyperlipidemia, and/or debilitating arthritis.1,3 Patients should have failed attempts to achieve a healthy weight loss or have been unable to sustain weight loss through other means.3 The National Institutes of Health, American College of Surgeons, and American Society for Metabolic and Bariatric Surgery recommend that surgery be performed by a board-certified surgeon with specialized training in bariatric surgery, to include a specialized team with a nutritionist, exercise specialist, and a mental health professional.3
THE PROCEDURES
The most commonly performed bariatric procedures are the Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy (SG), adjustable gastric band (AGB), and biliopancreatic diversion with duodenal switch (BPD/DS).3,4 Although traditionally done as open procedures, currently all procedures can be done laparoscopically.
Other, less common, procedures include the gastric balloon, V-block therapy, and the Aspire Assist device.4
Roux-en-Y Gastric Bypass
The RYGB is considered the gold standard of weight loss procedures and has been the most widely performed. First, a small pouch that holds approximately 30 mL is created from the upper portion of the stomach, with the remaining portion of the stomach divided off. The small intestine is then divided, and the bottom portion is attached to the small stomach pouch. The final step is attaching the top portion of the small intestine further down the ilium, allowing the gastric juices and pancreatic enzymes from the bypassed stomach, pancreas, and bile duct to eventually mix with food.3,4 (See Figure 1.)
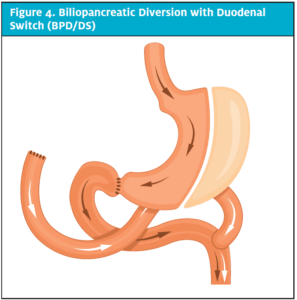
Figure 1. Roux-en-Y Gastric Bypass
This procedure causes weight loss by decreasing stomach volume, which causes early satiety; fewer calories to be absorbed from the bypassed small bowel; changes in gut hormones that reduce hunger; and reverse mechanisms of type 2 diabetes.3 Most patients will lose 60% to 80% of their excess weight and maintain 50% of the weight loss.4
RYGB may result in more complications than other procedures, lead to vitamin and mineral deficiencies (including iron, B12, calcium, and folate), require a longer hospital stay, and require strict patient adherence to diet and nutrient supplements.3
Sleeve Gastrectomy
The SG is done laparoscopically by removing approximately 80% of the stomach, leaving a tubular pouch. (See Figure 2.) This reduces intake by reducing volume and, thus, caloric intake. This procedure also has an effect on gut hormones and changes hunger, satiety, and blood sugar control. It is as effective as the RYGB procedure in terms of weight loss and remission of diabetes. The complication rate is less than that of gastric bypass, but disadvantages are that it is nonreversible and has the potential for vitamin deficiencies. Patients lose >50% of their excess weight and maintain about 50% of the lost weight off over time.3,4
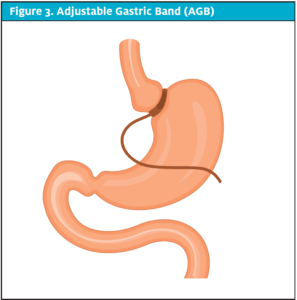
Figure 2. Gastric Sleeve (GS)
Adjustable Gastric Band
AGB is performed by applying a band around the stomach, filled with saline and that can be adjusted by gradually decreasing the diameter of the band and restricting the flow of food through the stomach. (See Figure 3.) Patients experience reduction of hunger and early satiety but still absorb calories and nutrients as before. These patients lose 40% to 50% of their excess weight.4 There is no cutting or rerouting involved, and it is reversible. Weight loss, however, is slower, bands can slip or erode, and patients can stretch the esophagus or stomach if they overeat. The highest rate of reoperation occurs with this procedure.3
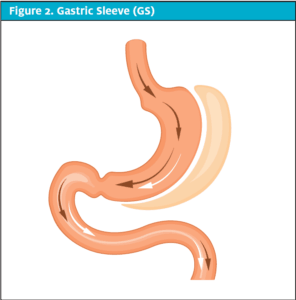
Figure 3. Adjustable Gastric Band (AGB)
Biliopancreatic Diversion with Duodenal Switch
A BPD/DS is initiated in the same way as a gastric sleeve, but the intestine is divided and diverted similarly to the RYGB. The stomach empties directly into the distal small intestine, where it is joined by the pancreatic and biliary secretions from the proximal small bowel. (See Figure 4.) This results in less food intake and less absorption of calories and nutrients, and affects the gut hormones. This is the most effective surgery for patients with diabetes, and has the most reported weight loss of 60% to 70% of excess weight which remains at 5 years. Fat absorption is reduced by 70%.4 However, this procedure also has the highest mortality and complication rate of all the procedures and is the most likely to result in deficiencies of protein, vitamins, minerals, calcium, zinc, and fat-soluble vitamins.3
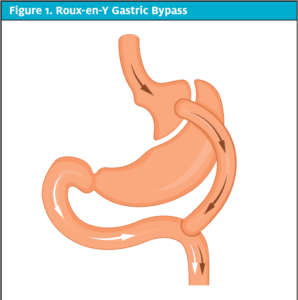
Figure 4. Biliopancreatic Diversion with Duodenal Switch (BPD/DS)
Postsurgery Nutrition
In all procedures, the patient with a now tiny stomach must comply with a diet plan gradually advancing from clear liquids to a stabilization diet. (See Table 1.) Failure to comply may result in complications. In the long term, patients are required to eat a high-protein diet, eat small meals, eat and drink as slowly as possible, and are encouraged to eat healthy fruits and vegetables. Patients should maintain hydration, but should not drink fluids immediately before, during, or after meals, only between meals. Noncompliance with dietary restrictions results in nausea and vomiting, stretching of suture lines and enlargement of the gastric pouch, abdominal pain, constipation, obstruction, and dumping syndrome.
Table 1. Post Bariatric Surgery Diet Plan
| Phase | Gastric Bypass | Gastric Band |
| Clear liquid diet | Weeks 1-2 | Week 1 |
| Full liquid diet | N/A | Week 2, add protein supplements |
| Pureed diet | Weeks 3-4, add protein supplements | Week 3 |
| Adaptive/soft diet | Months 2-3 | Weeks 4-5 |
| Stabilization diet | Month 4 and lifelong | Week 6 and lifelong |
COMPLICATIONS
Overall, the risk of mortality for these procedures is 1%, with a risk of serious complications of up to 10%.1 Patients more likely to have complications include males, ages >65, low functional status, open procedures, and a low-volume surgeon or low-volume hospital.6 The complications can be divided into postoperative, the first few days after surgery, short-term, days to weeks after surgery, and long-term, weeks to years after surgery.
Postoperative period
In the postoperative period, pulmonary emboli (PE), anastomotic leaks, and respiratory failure account for 80% of the mortality-related complications and are usually seen within 30 days of the procedure.
- The leading cause of death following bariatric surgery is PE.1,7
- Anastomotic leaks may present as persistent tachycardia, fever, rigors, hypotension, and severe abdominal pain, although pain is not required.7 The patient may present with sepsis syndrome. Patients with suspected leaks should have a gastrografin contrast study with prompt surgical consultation. Exploratory laparotomy may be the only way to diagnosis a suspected leak.1
Short-term
Short-term complications include vomiting, wound infections, stomal stenosis, marginal ulceration and constipation.1
- Wound infections are more common in patients who have had open procedures.8 Signs of infection include fever, pain, erythema, and purulence around the wound. These may occur up to 3 weeks after surgery in morbidly obese patients and should be treated aggressively with drainage and broad-spectrum antibiotics with MRSA coverage, if suspected. Wound infections may also result in incisional hernias.1,8 Seromas may also occur but are usually painless, nonpurulent, and not associated with fever or erythema.
- Vomiting is common following bariatric surgery and may at any time after the procedure. Although in most cases vomiting is due to overeating and dietary noncompliance, an organic cause should be sought if the patient is intolerant to liquids. Stomal stenosis may occur in up to 20% of RYGB patients, resulting in persistent vomiting. The diagnosis may be made by UGIS and can be improved by endoscopic dilation of the stenosis.1 Recurrent vomiting is more common following gastric band procedures. Severe cases may need IVF and TPN until they are able to tolerate oral feeds. Patients who frequently overeat may cause dilatation of their distal esophagus, causing regurgitation and nocturnal aspiration similar to achalasia.4
- Marginal ulceration may occur along the anastomotic site in up to 16% of patients.1,4 They may present as a GIB with hematemesis, melena, and orthostatic hypotension. Contributing factors include acid production by the gastric pouch, Helicobacter pylori infection, stress, and the use of nonabsorbable sutures.4 This may occur as both early and late complications. Early hemorrhage can occur from any of the staple lines or anastomoses sites. An endoscopic evaluation should be performed to identify the ulcer. NSAIDs increase this risk and should be strictly avoided in bariatric patients.1
- Postoperative constipation is common and results from narcotic pain medication (as NSAIDs are contraindicated), dehydration, and malabsorption. Patients should be hydrated and treated with stool softeners, laxatives, or enemas as indicated. Granular bulking agents should be avoided, as they may result in esophageal obstruction.1
Long-term
Long-term complications include cholelithiasis, postprandial hypoglycemia, dumping syndrome, persistent vomiting, and nutritional deficiencies.1
- Cholelithiasis and cholecystitis are common complications following rapid weight loss and may occur in up to 50% of these patients. In many cases, surgeons will perform prophylactic cholecystectomies during the bariatric procedure to prevent this. Bile salt administration may reduce this risk if the gall bladder remains.
- Postprandial severe hypoglycemia has been reported and thought to be due to pancreatic islet cell hyperplasia post bypass. Inappropriate insulin secretion may also occur. There is no specific treatment for this condition, only awareness and dietary modification.
- Dumping syndrome occurs due to the influx of undigested carbohydrates into the jejunum causing procholinergic symptoms such as nausea, vomiting, diarrhea, tachycardia, and dizziness. It is a complication of RYGB and BPD/DS that occurs after dietary noncompliance. It is self-limited and resolves after several hours of consuming sweets or foods high in sugar. Patients should avoid these items to prevent the syndrome.
- Vague complaints of abdominal pain may occur after any abdominal procedure. Obstruction is more likely to occur after laparoscopic gastric bypass rather than open procedures and may occur weeks to months after surgery. Internal hernias may also occur and are more frequent following a laparoscopic bariatric procedure.4
- Strictures may occur at any site of anastomosis resulting in food intolerance, vomiting, and abdominal pain. The incidence of this at the gastrojejunostomy site appears to be higher in the laparoscopic procedures.4 Technical errors, anastomotic leaks, ischemia and fibrosis may be responsible for the formation of strictures. Balloon dilatation may be required.
- The most frequent complication of the gastric band is “slippage” or prolapse of the stomach superiorly through the band. This causes obstruction of the lumen of the band and is associated with vomiting and gastroesophageal regurgitation. The misplaced band may be visible on radiographs. Any of the procedures that involve implantation of a foreign body to the external surface of the stomach can cause erosion through the gastric wall. This may be acute or chronic. Patients may present with abdominal pain, fever, signs of localized infection, or may have vague or no symptoms at all.4 Failure or disconnection of the port have also been described.
- Nutritional deficiencies are common after the malabsorptive procedures. Adherence to a high-protein diet is essential. Lifelong supplementation with a high-potency multivitamin, B12, and calcium should be continued. Some menstruating women may require parenteral iron supplementation due to poor absorption of enteral iron. Acute encephalopathy caused by thiamine deficiency has been reported.4
- A very small group of patients may develop protein malnutrition months to years following surgery due to anastomotic strictures, food phobias, or simply failure to consume enough protein. Alopecia is a relatively common early finding of protein malnutrition.4 These patients will have repeated episodes of nausea and vomiting and dehydration, and may have renal or hepatic insufficiencies. Treatment includes TPN, dilatation of their strictures, if present, and re-education regarding proper diet until malnutrition has resolved.1
LIFESTYLE, MEDICATION, AND DIETARY CHANGES
For the first 1 to 2 months following surgery, patients may require liquid medications. Medications that do not come in liquid form can be crushed and mixed with liquid or sugar-free pudding or applesauce. Once the patient has progressed to a stabilization diet, pills can again be used. Larger pills may need to be broken or crushed.
Bariatric patients should be instructed to avoid NSAIDs for life1,2,5 due to their high risk of GI bleeding and marginal ulcers. Patients should be instructed about specific names including brand names as well as common over the counter names. Many other specialties, for example dentists and podiatrists, are unaware that NSAIDs should be avoided, so patients need to be well educated and vigilant about taking them. Anti-osteoporosis medications and steroids should be avoided for the same reason. If absolutely necessary, steroids can be given with a PPI to prevent bleeding. Granular bulking agents used to add fiber and for constipation may cause obstructions and impaction in the esophagus1,5 and in the intestines and should be avoided.
Controlled-release medicines should be avoided. The altered absorption and production of digestive enzymes can make their release unpredictable and patients may not receive the intended dosage.5
Clinicians should be aware that as a patient’s weight drops, they may note regression in their hypertension and diabetes, requiring lower doses of their current medications. Suspect this if patients present with hypotension, bradycardia, or hypoglycemia without another explanation. Toxicity at lower doses of other previously prescribed medications, such as psychiatric medications may also occur.
Nicotine increases the risk of GIB; patients should be encouraged not to smoke. Similarly, alcohol increases the risk of bleeding and also may have increased absorption causing sensitivity to even small amounts.
Certain foods should also be avoided due to their difficulties with digesting in both the stomach and absorption in the intestines. (See Table 2.)
| Table 2. Foods to Avoid After Bariatric Surgery |
| Nuts and seeds |
| Popcorn |
| Dried fruits |
| Carbonated beverages |
| Granola |
| Stringy or fibrous vegetables (celery, corn, cabbage) |
| Tough meats or gristle |
| Fried foods |
Pregnancy is not recommended until 12-18 months after surgery due to nutritional deficiencies and inability to take in enough protein to support a growing fetus. Patients should be counselled to avoid pregnancy and may need birth control. Patients who become pregnant in the early months following bariatric surgery should be referred to an obstetrician immediately for careful monitoring.9
SKIN CHANGES POSTSURGERY
Skin issues are common after massive weight loss. Most patients will need skin reduction surgery. Nutrient deficiencies can cause a variety of skin disorders (Table 3), as well as poor wound healing and reduced resistance to infection. Damage to elastin fibers and collagen from stretching followed by weight loss can also occur and make the loose skin behave differently when surgery is performed.
| Table 3. Long–Term Skin Changes Due to Nutrient Deficiency after Bariatric Surgery | |
| · Acne | · Glossitis |
| · Alopecia | · Pellagra |
| · Angular cheilitis | · Psoriasis |
| · Burning feet syndrome | · Seborrheic dermatitis |
| · Depigmentation | · Toxic epidermal necrosis |
| · Eczema | · Xeroderma |
| · Erythroderma | |
Approximately 90% of patients will have negative effects secondary to large amounts of redundant skin. These may include aesthetic issues, functional problems, and dermatosis, as well as difficulties with personal hygiene.8 Chafing may occur due to layers of skin rubbing against each other causing irritation, dryness, and pain. Moisturizers such as Aquaphor, Eucerin, and commercially available skin lubricants may improve these symptoms.
Intertrigo or intertriginous dermatitis appears between skin folds as a moist erythema. It may be malodorous and weeping. It is usually itchy and tender. Friction between deep skin folds and absence of air circulation causes this rash to occur. This may be complicated by candida or bacterial infection. Irritant or contact dermatitis may exacerbate the condition. Fungal elements can be identified with a KOH prep or Wood’s lamp. Erythrasma is a cutaneous corynebacterial infection presenting as red or brown macerated, scaly plaques that fluoresce red under Wood’s lamp.10
Skin fold disorders should be treated and prevented by washing the area daily with soap and water, then drying meticulously. A hair dryer on low setting may be used. Daily aeration of the affected area and application of drying powders are recommended. Absorbent clothing or layers of cloth to separate skin folds may also help.10 Fungal infections should be treated aggressively with combination antifungal and steroid creams. Erythrasma should be treated with topical clindamycin or erythromycin. If cellulitis is present, oral antibiotics are necessary. Diabetes should be tightly controlled. Severe or recurrent cases should be referred for skin reduction surgery.
TAKE-HOME POINTS
- Post bariatric surgery patients are becoming more commonplace in the urgent care setting.
- NSAIDs should never be prescribed to these patients .
- Suspect overeating or dietary noncompliance when patients present with vomiting. If they are also intolerant to liquids, the patient should be evaluated for an organic cause.
- The most common complications in the first month postprocedure are pulmonary embolus and anastomotic leaks, and require a high index of suspicion.
- Wound infections should be treated aggressively to prevent systemic infections and subsequent hernias.
- As weight loss occurs, patients may present with hypotension or hypoglycemia as their hypertension and diabetes regresses.
- A Wood’s lamp may be used to identify fungal infections and erythrasma when there is a rash between skin folds
References
- Virji A, Murr MM. Caring for patients after bariatric surgery. Am Fam Physician. 2006;73(8):1403-1408.
- Centers for Disease Control and Prevention. Obesity and overweight. Available at: https://www.cdc.gov/nchs/fastats/obesity-overweight.htm. Accessed February 11, 2020.
- American Society for Metabolic and Bariatric Surgery. Available at: asmbs.org. Accessed February 11, 2020.
- Elder KA, Wolfe BM. Bariatric surgery: a review of procedures and outcomes. 2007;132:2253-2271.
- Geraldo MDP, Fonseca FLA, Gouveia MR, et al. The use of drugs in patients who have undergone bariatric surgery. Int J Gen Med. 2014;7:219-224.
- Nguyen NT, Masoomi H, Laugenour K, et al. Predictive factors of mortality in bariatric surgery data from the Nationwide Inpatient Sample. Surgery. 2011;150(2):347-351.
- Flum DR, Salem L, Elrod JA, et al. Early mortality among Medicare beneficiaries undergoing bariatric surgical procedures. 2005;294(15):1903-1908.
- Halawi A, Abiad F, Abbas O. Bariatric surgery and its effects on the skin and skin diseases. Obes Surg. 2013;23:408-413.
- Kominiarek M. Preparing for and managing a pregnancy after bariatric surgery. Semin Perinatol. 2011;35(6):356-361.
- Kalra MG, Higgins KE, Kinney BS. Intertrigo and secondary skin infections. Am Fam Physician. 2014;89(7):569-573.
Tracey Quail Davidoff, MD, FCUCM is an Attending Physician at Advent Health Centra Care in Orlando, FL. The author has no relevant financial relationships with any commercial interests.
