Published on
The Resolution
Differential diagnosis:
- Ventricular tachycardia
- Atrial flutter
- Supraventricular tachycardia
- Atrial fibrillation
- Multifocal atrial tachycardia
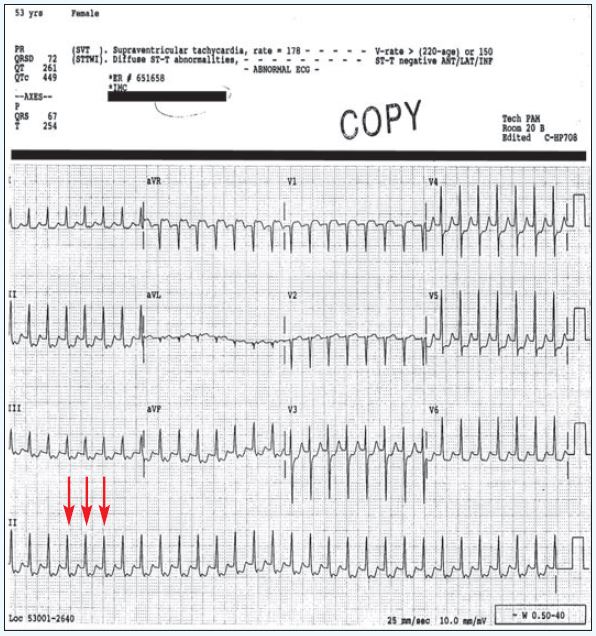
Diagnosis
This patient has supraventricular tachycardia (SVT). The ECG reveals a tachycardic rate; the rhythm is regular, excluding atrial fibrillation and multifocal atrial tachycardia. There are no flutter waves, making the diagnosis of atrial flutter unlikely (also, the atrial flutter rate is typically 150). The QRS complexes are narrow, excluding ventricular tachycardia. P waves are not seen. The tracing is most consistent with supraventricular tachycardia. There are some ST depressions which could be a rate related ischemia. These generally resolve with the management of the SVT.
Learnings
- SVT is a regular, narrow complex and tachycardia rhythm
- The mechanism is a re-entrant tachycardia
- Distinguish from atrial fibrillation (irregular, irregular rhythm), atrial flutter (flutter waves and typical rate of 150), ventricular tachycardia (wide complex QRS), and sinus tachycardia (presence of p waves)
- Symptoms may include sensation of palpitations, lightheadedness, shortness of breath, chest pain, or weakness
Pearls for Initial Management and Considerations for Transfer
- Unstable patients displaying hypotension, confusion, diaphoresis, or chest pain should have an IV placed and be put on the monitor (if time allows), then transferred to an emergency department
- Stable patients may attempt the Valsalva maneuver by “bearing down” or postural modification by having the patient Valsalva, then having the clinician perform a passive leg raise
- Emergency department management will initially proceed with adenosine administration, while unstable patients may require cardioversion
Clinical Challenge 2: October 2017
1 2