
Urgent message: Giant cell arteritis is an under-recognized and easily missed vasculitis of older adults, a challenging but “can’t miss” diagnosis. The urgent care clinician must be able to recognize this entity sometimes referred to as the “great masquerader” and be comfortable initiating timely emergency treatment.
Ryan C. Jacobsen MD, EMT-P
Giant cell arteritis (GCA), more commonly known as temporal arteritis, is an under-recognized vasculitis of older adults that can have potentially devastating consequences, most notably permanent and profound vision loss, if missed.
In addition to remaining vigilant for symptoms of this entity sometimes referred to as the “great masquerader” and being comfortable initiating timely emergency treatment, the clinician must appreciate the importance of timely involvement of the appropriate subspecialty consultants in the care of these patients.
This article will provide the urgent care specialist with an overview of the disease, various clinical presentations, laboratory tests that assist in making the diagnosis of giant cell arteritis, and guidance on management.
Epidemiology
GCA is the most common, primary systemic vasculitis occurring in adults.1 Due to the lack of any pathognomonic clinical presentation and the large number of non-specific complaints that GCA patients can present with, the incidence and prevalence of the disease is almost certainly underestimated.2 Prevalence on autopsy studies is reported at 1.2% of the population.2
Overall, global incidence has been placed at 15 to 25 per 100,000/year in individuals over 50 years of age.3 However, the incidence varies dramatically based on age, geographic location, race and sex.
GCA is extremely rare in individuals under 50 years
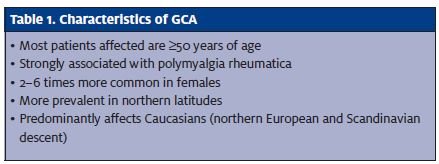
of age.1,2,4 The incidence rises from 2.3 per 100,000/year in individuals in their 60s to 44.7 per year in their 90s.5 Peak incidence occurs between 75 and 80 years of age.2,6 It is more likely to occur in Caucasians, especially those of Scandinavian and Northern European descent. It is uncommon in African Americans, and rare in the Hispanic population.
Also, it is two to six times more likely to afflict females than males.2,5
Long-term outcome studies have shown no excess in mortality; however, delays in diagnosis and initiation of treatment contribute to the high morbidity associated with GCA.7
Pathophysiology
GCA is a systemic inflammatory vasculitis that mainly affects the proximal aorta and its branches.3,5,8 This vasculitis predominantly targets the muscular walled, medium to large arteries of the head and neck.2,5,7 How- ever, there is evidence that this particular vasculitis, al- though much less frequently, can also affect other arter- ies such as: the mesenteric arteries, coronary arteries, and branches off the distal aorta including arteries of the lower extremities.5,9,10
Although not proven definitively, many triggers have been postulated for GCA, including:
- heavy smoking
- atherosclerosis
- cytomegalovirus (CMV)
- herpes
- parainfluenza
- parvovirus B19
- mycoplasma
- 5,7
The exact immunological mechanisms and triggers that occur in GCA are not completely understood.2,5 However, some believe that the systemic inflammatory response of GCA is mediated by the innate immune sys- tem (i.e., non-antigen mediated) and that damage is caused by a maladaptive antigen-specific immune re- sponse that directly attacks the arterial walls. 10
Regardless of the triggers and immunological mechanisms that are involved, however, the ultimate result is arterial wall inflammation. This leads to occlusion of the arterial lumen, resulting in ischemia distal to the occlusion. Ischemia is the primary cause of the wide array of clinical signs and symptoms seen in GCA and is the culprit behind the most commonly encountered, serious consequence: vision loss.2,5,8,10 Typically, the vision loss associated with GCA is a consequence of ischemia of the optic nerve, most likely due to widespread inflammation and luminal occlusion of the posterior ciliary arteries that supply the optic nerve head. This is usually referred to as anterior ischemic optic neuropathy (AION), and is the most common ocular manifestation of GCA. 9,11 GCA can also cause a host of other ischemic complications that can affect vision, including central retinal artery occlusion (CRAO), posterior ischemic optic neuropathy, choroidal ischemia, and branch retinal artery occlusion.2,8,9,12 Other ischemic manifestations can include: aortic arch syndrome (resulting in claudication of upper extremities), aortic dissection/aneurysm, transient ischemic attack/CVA, acute coronary syndromes (ACS), mesenteric ischemia, and ischemia/infarction of muscles of mastication, pharyngeal musculature, and tongue.2,5,8,13 Association between polymyalgia rheumatica (PMR) and GCA is strong; up to 40% of patients with GCA have PMR, as well,6,7,10 but only about 15% of patients with PMR have GCA.
PMR is another systemic inflammatory disease that presents with myalgias of the neck, shoulders, and pelvic girdle. Typically, the symptoms of PMR are worse in the morning after waking, and are frequently accompanied by non-specific complaints such as fatigue, malaise, fever, weight loss, and anorexia.6,7
Clinical Presentation
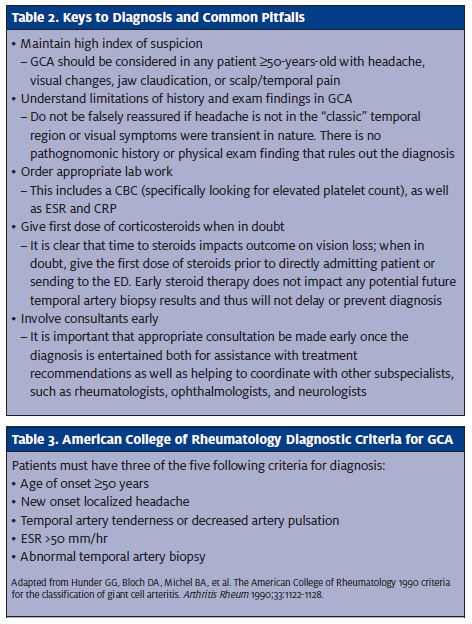
It is important to understand that there are no pathognomonic clinical signs or presenting symptoms for GCA.2,6-8,10,13 The clinician needs to be familiar with the more common presenting signs and symptoms. We must also realize that the diagnosis of GCA can be very challenging due to the sometimes vague, non-specific symptomatology. Therefore, clinicians must keep a very high index of suspicion for disease in the appropriate patient. Headache is the most common complaint, occur- ring in roughly 90% of patients.2 However, the headache does not have to be temporal in location. The headache of GCA can be parietal, occipital, generalized, acute, or subacute in nature.7,14 Ocular complaints are common, ranging in incidence from 14% to 70% of patients.3 Visual loss is the most common ocular complaint reported, occurring in up to 98% of patients, followed by diplopia in 6% to 21% of patients.2
The clinical presentation for arteritic anterior ischemic optic neuropathy (A-AION) is acute, painless, monocular vision loss. The presence of any visual complaint, however, should heighten suspicion of GCA in any patient over 50-years-old.
Such complaints include:
- transient visual loss
- ocular pain
- visual blurring
- amaurosis 5
In one prospective study, vision loss was the only symptom in 21% of patients diagnosed with GCA. 12 The importance of taking all visual complaints seriously in older patients, even if transient, cannot be overstated as these may be the only clues to the disease which, if missed, can result in permanent blindness.
Jaw claudication has been reported to be very specific and quadruples the likelihood of diagnosis but only occurs in 30% to 50% of patients with GCA, making it extremely insensitive.2,4,7
It is important to differentiate between jaw claudication and temporomandibular joint pain (TMJ). Jaw claudication begins after several minutes of chewing or talking, subsides with rest, and is located over the temporal region. TMJ pain is immediate with any jaw movement at all and is located primarily directly over the temporo- mandibular joint just in front of the ear.2
Scalp tenderness can be seen in approximately 50% of patients with GCA. The patient may note pain with hair washing, brushing, or even lying on a pillow. Some may describe this as having “painful hair.”7
There are a multitude of non-specific complaints. About 65% of patients report an alteration in general well-being.2 Other systemic complaints can include:2,4,5,7,14
- fever (generally low grade)
- anorexia
- weight loss
- malaise
- fatigue
- paresthesias
- joint pain
- dizziness
- hoarseness
- dysphagia
Key Physical Exam Findings
There are no findings on physical exam that are pathognomonic for GCA. However, there are several findings that increase the likelihood of identifying GCA. The clinician should be able to recognize these key findings. Temporal artery abnormalities of any kind on physical exam double the likelihood that a patient has GCA. This can include tenderness when directly palpating the artery, beading of the artery, an abnormally prominent artery, or absence of temporal artery pulses.14
The other classic physical exam clue that can be present in GCA is fundoscopic findings of AION. It is important to do a fundoscopic exam, when feasible, to look for the telltale signs of ischemic retinopathies.
The typical appearance of AION is a chalky white, pale, swollen optic nerve head and/or cotton wool hemorrhages. Other possible findings include afferent pupillary defects and visual acuity test- ing abnormalities.5,9,12,14
Palpation of the scalp is also an essential physical exam maneuver; pain secondary to scalp ischemia may be evident in up to 50% of patients with GCA.7
Outside of the above physical exam clues, there are no “typical” findings for patients presenting in the urgent care setting. Therefore, it is important for the clinician to not dismiss GCA as a potential diagnosis in the absence of any of the above findings.
Differential Diagnosis
Again, PMR is another systemic inflammatory condition that frequently coexists in patients with GCA. Any systemic inflammatory disease can mimic GCA; likewise, GCA can mimic any systemic inflammatory disease. Therefore, the differential consists of many conditions that have non-specific symptoms like fever, weight loss, fatigue, myalgias, and arthralgias (thus, the reason some refer to GCA as “the great masquerader”).
Some differentials that also present with non- specific complaints are:
- fibromyalgia
- rheumatoid arthritis
- migraine headache
- lupus
- viral infections
- hepatitis
- endocarditis
- HIV
- malignancy
- sinusitis
- osteoarthritis
- polymyositis,
- other 6,7
Diagnosis
It is important to understand that there is no single lab- oratory test or imaging study that is specific for GCA.5 There are, however, certain tests that should be obtained in any patient over 50-years-old who you suspect of having GCA. These are a sedimentation rate (ESR), C- reactive protein (CRP), and complete blood count (CBC).2,4-8
ESR
Historically, the ESR has been the gold standard labora- tory test to assist in the diagnosis of GCA; it has been used for decades.
Approximately 85% of patients with GCA will have an elevated ESR, >50 mm/hour.13
While strongly supportive of GCA, it is negative in up to 17% of GCA cases and thus is insensitive for ruling out the disease.15
Another major limitation of the ESR is the extreme non-specificity of an elevated test. Any inflammatory/infectious condition, as well as increasing age, can cause elevation in the ESR. Other conditions that raise the ESR are female sex, connective tissue disorders, anemia, hypercholesterolemia, and trauma. Despite its limitations most authors still recommend the use of the ESR in the laboratory evaluation of GCA.2,5-8,14,15
CRP
The CRP is an acute phase reactant that is released by the liver in response to a wide variety of inflammatory/infectious stressors.5 The CRP has become an important di- agnostic laboratory test in the evaluation for GCA. An elevated CRP has a reported sensitivity of up to 97.5% to 100% for active GCA.2,16,17 CRP also has distinct advantages over the ESR in that it does not elevate for age, anemia, and sex like ESR does.2,5
CRP and ESR
When used together, the combination of ESR and CRP has a reported sensitivity of over 99% for identifying patients with GCA, as well as a specificity of 97%, and is therefore a very important part of the work-up in excluding GCA in pa- tients.16,17
CBC
The most important element in the CBC when evaluating a patient for GCA is the platelet count. Thrombocytosis (platelet count >400 x 103/μL) may be present in 50% to 60% of patients with biopsy- proven GCA.18,19 This makes the platelet count a useful laboratory test for GCA, as thrombocytosis carries with it both high specificity (91%) and a high positive predictive value (87%).19
Again, it cannot be used to rule out the disease due to low sensitivity. 2,5,19
Many patients with GCA will have a normocytic, normochromic anemia, as well. However, this is an in- credibly non-sensitive and non-specific finding and should not be relied upon as evidence for or against the diagnosis of GCA.2,5,7,8
Imaging modalities specific to assisting in diagnosis of GCA
There are no gold standard imaging studies that need to be performed in the urgent care or emergency department setting. They should generally only be ordered at the discretion and guidance of subspecialty consultants.
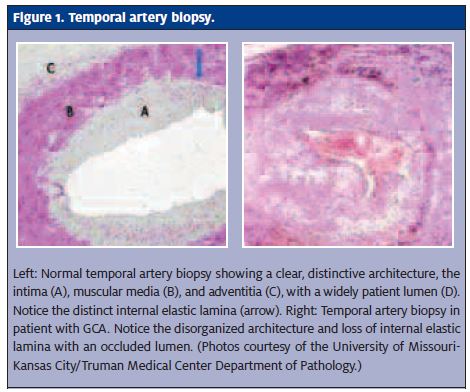
Temporal artery biopsy
Finding histological evidence of giant cell arteritis on biopsy of the temporal artery is the gold standard for diagnosis of the disease and should be done on any patient over 50 years of age when there is the slightest suspicion for the disease.1,5,7,8,10,13 As will be discussed in the management section, it is important to attempt to confirm the diagnosis before beginning treatment, due to the untoward side effects of potential long-term steroid therapy. Even so, unfortunately, the sensitivity for biopsy is only 87%.5
In 1990, the American College of Rheumatology (ACR) developed diagnostic criteria that were 94% sensitive and 91% specific for the diagnosis of GCA if three out of the five criteria were met (Table 3).4,8
However, some are concerned that the ACR’s recommendations do not in- corporate important findings such as visual symptoms, jaw claudication, scalp tenderness, and elevated CRP into the decision making process.5 Thus, the ACR’s guidelines by themselves should not be considered adequate to exclude the disease entirely. Rather, they may be helpful in pointing out high-risk patient characteristics.
It is not necessary to have biopsy proven GCA in order to diagnose and treat the disease. In the literature, it is sometimes referred to as biopsy positive and biopsy-negative GCA.
If clinical suspicion is high enough in the appropriate patient, treatment will frequently be continued regardless of the biopsy results. This is necessary due to the insensitivity of temporal artery biopsies, as well as the potentially disastrous consequences of withholding therapy.1,2,20
Management
The overwhelming guiding principle in management of GCA is to halt the inflammatory process and attempt to prevent the morbidity associated with ischemic complications, such as permanent vision loss.2,5,7,8,20 Other potential complications seen in patients with GCA can include subclavian steel syndrome, arm claudication, and thoracic aneurysms (which can occur up to 15 years after the diagnosis of GCA is made).
Corticosteroids
The gold standard treatment in the management of GCA is corticosteroids. While there have been no universally accepted recommendations on dosing, route of administration, and length of treatment, there is one point that is agreed upon by nearly all authors: the prompt initiation of treatment.2,5,8,20
Clinicians may be reluctant to place a patient on steroids for fear of interfering with biopsy results that may be done in the future. This concern is unfounded, however, as there is evidence that histological findings of disease are present up to six weeks after steroids are initiated. 21
Treatment with steroids should be started as soon as the diagnosis is entertained. GCA does not require a histological diagnosis or any other confirmatory lab/imaging study in order to give the first dose of steroids. The importance of early treatment was demonstrated by one study that revealed when steroids were begun within 24 hours of symptom onset, visual symptoms improved in 57% of patients, compared with only 6% of patients improving when treated outside the 24-hour window. 22
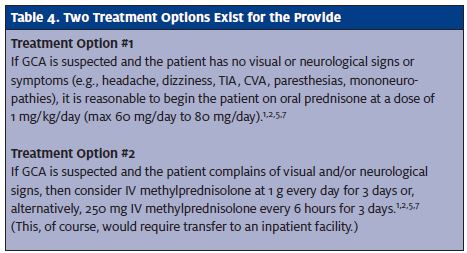
Several different steroid regimens to treat GCA have been suggested by various resources and authors. The urgent care provider should not worry about the specific recommendations, as many deal with duration of treatment (months versus years), tapering dosages, and various steroid alternatives such as methotrexate and TNF-alpha inhibitors. All of these should be managed by the subspecialty consultants who will follow the patient over time.1,2,5,7
There are generally agreed-upon principles of management that the clinician can use to guide treatment, however, as highlighted in Table 4.
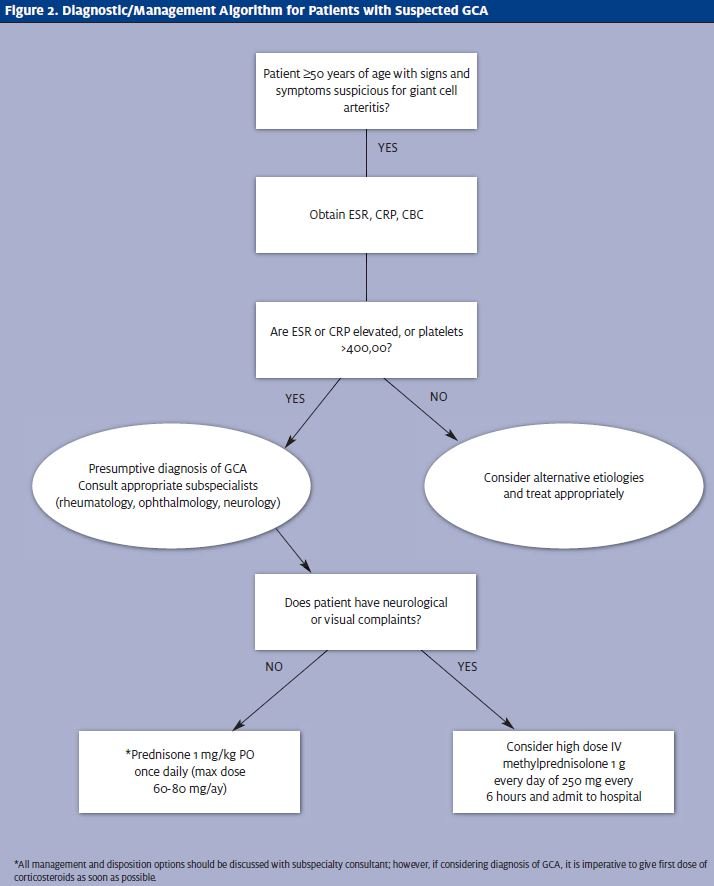
The general consensus in the literature is that there is no strong evidence to support one route over the other (IV versus PO), but these recommendations are generally agreed upon by most authors.20
Consultation
Subspecialty consultant guidance should be obtained early in the patient encounter, as soon as the diagnosis of GCA is entertained. Rheumatology, ophthalmology, and neurology are appropriate consultants to involve, depending on the patient presentation. However, a rheumatologist usually guides management over the long term, as patients are typically treated with steroids for many months (and frequently for years).1,2,5-7
Consultants will be able to help guide decision making on disposition and follow-up; however, most patients placed on high-dose steroids for the suspicion of GCA are admitted to the hospital to observe for complications of such treatment, as well as concerns over diagnostic uncertainty.
Another indication for direct admission or transfer to an ED is any concern over compliance with the treatment regimen. Providers should be wary of sending older patients home without first confirming the patient’s ability to obtain medication, adequate transportation to follow-up appointments, and a sufficient social support system in place to encourage compliance with therapy.
Patients with other comorbidities, especially diabetes, should also be transferred to an ED or admitted directly through a consultant, as high-dose steroids will likely result in worsening disease which will benefit from in-hospital monitoring.
The complications arising from steroid use are well known and consultants will be invaluable in determining the appropriateness of alternative therapies such as methotrexate and TNF-alpha blockers, among others. These treatments have not gained widespread acceptance yet and should only be instituted under guidance from consult- ants and will rarely occur in the acute setting.1,2,5-7
Conclusion
GCA can be an elusive and challenging disease to diagnose. As such, clinicians should be vigilant for its signs and symptoms, and diligent in asking, “Could this patient have GCA?” Specifically, we should be suspicious in any patient over 50-years-old who has non-specific complaints such as alteration in well-being, new headaches, scalp or temporal pain, and visual com- plaints, as prompt treatment is necessary to avoid potentially devastating consequences.
References
- Mukhtyar CL, Guillevin MC, Cid B, et EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis. 2009;68(3):318-323.
- Kawasaki A, Purvin Giant cell arteritis: An updated review. Acta Ophthalmol. 2009;87(1):13-32.
- Hunder Epidemiology of giant cell arteritis. Cleve Clin J Med. 2002;69 Suppl 2:SII79- SII82.
- Nusser JA, Howard E, Wright Clinical inquiries. Which clinical features and lab find- ings increase the likelihood of temporal arteritis? J Fam Pract. 2008;57(2):119-120.
- Chew SS, Kerr NM, and Danesh-Meyer Giant cell arteritis. J Clin Neurosci. 2009;16(10):1263-1268.
- Unwin B, Williams CM, Gilliland Polymyalgia rheumatica and giant cell arteritis. Am Fam Physician. 2006;74(9):1547-1554.
