Urgent message: Close follow up is necessary for pediatric patients with vague presentations, lest a diagnosis of childhood cancer be missed.
JANET D. LITTLE, MD
Introduction
This case presentation reflects the challenge of diagnosing childhood cancers in a timely and accurate way. The presenting signs and symptoms are oftentimes nonspecific and can mimic those of common childhood conditions.1 The frequency of delayed diagnosis for childhood cancers is high, and reflects the importance of close follow-up instructions for patients with vague and non-specific presentations.
Case Presentation
A 12-year-old female with a past medical history signif- icant for mild-intermittent asthma presented to the urgent care center complaining of 3 episodes of nausea and vomiting, sore throat, mild shortness of breath, and chest discomfort. Her shortness of breath was not accompanied by a cough and was not relieved with use of her albuterol inhaler.
She had been seen by her dentist just 2 days prior to the onset of her symptoms for a dental abscess and was on penicillin, which she had taken numerous times before. She had decreased appetite at the onset of her symptoms. The patient denied any recent upper respi- ratory symptoms, abdominal pain, fever, chills, weight loss, fatigue, or rashes.
She was otherwise healthy with no known drug aller- gies. She took Albuterol as needed and Flovent for her asthma, which typically was triggered by environmen- tal allergens and exercise. Her mother noted that the child had pneumonia in the past. There was no other significant past medical, surgical, family or social history contributory to her presentation.
Observation and Findings
Physical examination of the patient revealed the following: T: 98.1oF
BP: 114/76 P: 100
R: 20
SpO2 98% on RA.
In general, the patient was a well-developed, well- nourished female in no acute distress, respiratory or oth- erwise. Examination of ENT, cervical lymph nodes, cardiovascular, respiratory, and skin were normal.
Diagnostic Studies and Differential Diagnosis
Laboratory tests were negative for rapid strep. Prelimi- nary reading of her chest x-ray was notable for lack of infiltrates and effusions, and normal cardiac size (Figures 1 and 2).
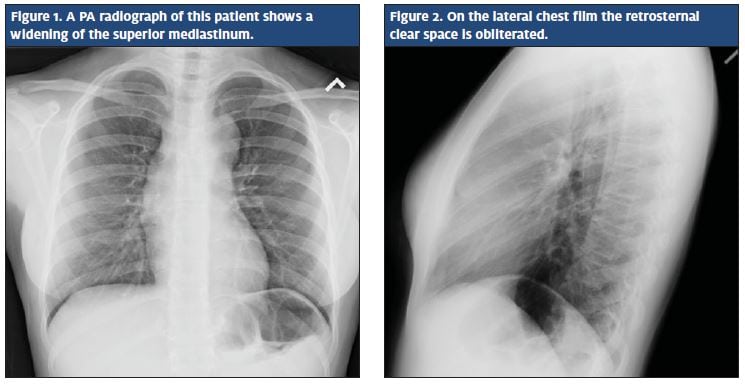
Differential diagnosis at the time included reaction to antibiotics or recent dental procedure. A less likely cause that was also considered was infective endocarditis seeded from her recent dental abscess/procedure. The mother was mostly concerned for pneumonia. The patient was discharged home with an antiemetic and recommendation for follow up in 1 day if her symptoms were not improving. The parent was also advised that a radiologist would do a final read of the chest x-ray and that she would be notified of the results.
The final chest x-ray report noted the lungs to be clear and the heart size within normal limits. However, there was a lobulated anterior mediastinal mass. Considera- tions included germ cell tumor, lymphoma, or thymic origin tumor. It was recommended that computed tomography (CT) with contrast be completed for further evaluation.
The patient was sent for a STAT CT scan of her chest 2 days after her initial visit. The preliminary report iden- tified a very large, confluent, anterior/superior mediasti- nal mass, approximately 10 x 8 x 3 cm. Differential diag- nosis: Lymphoma, thymoma (uniform non-enhancing tissue with no cystic area). The lungs were clear. Aside from the mass, no adenopathy was seen.
The patient and her family returned to the urgent care center to review the test results. At that time she reported feeling much better with the antiemetic but still had some shortness of breath. The case was dis- cussed with physicians at the nearest university hospital, to which care was then transferred.
Hospital Course (review of records obtained)
The patient was admitted by the university hospital pediatric sub specialty team for further evaluation. She was noted to have an approximately 2-cm nontender supraclavicular lymph node near the right sternal border.
Initial positron emission tomography/CT scans were notable for abnormally increased metabolic activity of a large multilobulated anterior mediastinal mass with associated mediastinal and supraclavicular lym- phadenopathy, consistent with Hodgkin Lymphoma without evidence of metastasis.
Bone marrow biopsy of the patient’s left hip showed no evidence of lymphoma. An excisional lymph node biopsy of the right supraclavicular node was also completed. Preliminary results were also concerning for Hodgkin Lymphoma. A final diagnosis of Stage IIA Hodgkin Lymphoma was given at the time of discharge 1 week later. The plan was to place a PICC line and per- form a bone marrow biopsy of the child’s right hip. The patient currently is undergoing chemotherapy and receiving outpatient care from the hematology/oncology service. It is believed that the large mediastinal mass will respond favorably to chemotherapy without the need for surgical excision at this time.
Discussion
Differential diagnosis of anterior mediastinal masses can be remembered by the 5Ts mnemonic:
- Thymus
- Thyroid
- Thoracic Aorta
- Terrible Lymphoma
- Teratoma and germ cell tumors
Hodgkin Lymphoma is a cancer of the lymphatic system of unknown eitiology. While Epstein-Barr virus has been associated with some cases of Hodgkin Lym- phoma, no specific link has been consistently impli- cated. The disease peaks in the teen years and then again in the third decade of life.2
Painless lymphadenopathy of the cervical, supraclavicular, and axillary lymph nodes is the most common presentation. Symptoms consistent with mediastinal mass include cough, chest pain and dyspnea. When these are combined with unexplained lymphadenopathy, especially supraclavicular or axillary, an urgent care provider should have a high index of suspicion and proceed with further investigation. Fever of unknown origin, night sweats, and weight loss are also frequent presenting symp- toms in Hodgkin Lymphoma as well as many other child- hood cancers, and should always be taken seriously.2
Conclusion
In this case, the patient presented with very non-specif- ic symptoms, demonstrating the difficulty of diagnosing childhood cancers, particularly because they are rare and oftentimes mimic other more common childhood illnesses. It is important for the urgent care provider to counsel patients about the importance of close follow up, especially when their symptoms are non-specific or incon- sistent with the presenting history.
References
- Young G, et.al. Recognition of common childhood malignancies. J Am Fam Phys. 2000;61(7):2144-2154.
- Glass Role of the primary care physician in Hodgkin lymphoma. J Am Fam Phys. 2008;78(5):615-622, 625-626.