Published on
Urgent Message: The accurate and prompt diagnosis of Kawasaki disease depends on clinicians’ familiarity with the diagnostic criteria and ability to recognize the waxing and waning manifestations of this pediatric condition.
Dominic K. Hardatt, DMSc, PA-C
Citation: Hardatt DK. Incomplete Kawasaki Disease Clinically Diagnosed from Urgent Care: A Case Report Based Review. J Urgent Care Med. 2024;18(5);34-39.
Keywords: Kawasaki disease, mucocutaneous lymph node syndrome, incomplete Kawasaki disease, febrile illness, fever, polymorphous rash, pediatric, coronary artery aneurysms, coronary artery dilatation
Abstract
Introduction
Kawasaki Disease (KD) is a panvasculitis condition that is the leading cause of coronary artery disease (CAD) and heart disease in childhood. It is a diagnosis that depends heavily on the clinician’s ability to recognize the clinical manifestations. Lab tests and other tests can aid clinicians with the diagnosis, but they do not confirm the presence of KD. The key to efficient diagnosis is recognizing the clinical diagnostic criteria for KD and promptly initiating treatment. The diagnostic criteria involves fever for at least 5 days and at least 4 out of the 5 additional clinical findings, with symptoms not explained by another diagnosis. If only 2 or 3 criteria are met with a fever for at least 5 days, incomplete KD can be diagnosed. Although KD can be a self-limited disease, morbidity and mortality can arise if children are inadequately treated. Complications of KD associated with delays in treatment include coronary artery aneurysms. Intravenous immunoglobulins (IVIG) and high-dose aspirin are the cornerstones of KD treatment.
Clinical Presentation
A 3-year-old boy presented to a local urgent care (UC) twice within a period of several days. He had fever at both visits and associated rash, conjunctivitis, lymphadenopathy, and oral involvement. Rapid testing for Strep pharyngitis, throat culture, and influenza viral testing were negative. The fever had persisted for 6 days by the time of his second visit and was not responsive to antipyretics.
Diagnosis, Interventions, and Outcome
Based on the clinical criteria for diagnosis, KD was confirmed at the second UC visit. The patient was referred immediately to a pediatric emergency department (ED). The hospital clinicians felt that the diagnosis of KD was appropriate, and the patient was admitted. He received IVIG and was discharged without any adverse events. At a 1 month cardiology follow-up, his echocardiogram was reassuring, and no apparent persistent cardiac consequences were evident.
Conclusion
The accurate and prompt diagnosis of KD depends heavily on clinicians’ familiarity with the diagnostic criteria and ability to recognize the commonly waxing and waning manifestations of this pediatric condition. While KD can be diagnosed clinically, signs and symptoms overlap with many self-limited illnesses for which children commonly present to UC. However, vigilance and consideration for KD are critical as early diagnosis dramatically reduces the risk of cardiac complications.
Introduction
Kawasaki disease, formerly known as mucocutaneous lymph node syndrome, is a panvasculitis condition affecting children most commonly under the age of 5. It was discovered by Tomikasu Kawasaki, MD, in 1967.1 Mucocutaneous lymph node syndrome gets its name because it typically affects mucous membranes, skin, lymph nodes, and blood vessels. Kawasaki disease received increased attention during the SARS-CoV-2 (COVID-19) pandemic given its relation to the multisystem inflammatory syndrome in children (MIS-C), a novel entity and uncommon, but serious complication of COVID in children. MIS-C consists of myocarditis, toxic shock syndrome, and KD.
While COVID-19 can lead to MIS-C, a Kawasaki-like illness, the etiology of KD remains poorly understood. Multiple candidate theories regarding the etiology have been proposed, including autoimmunity most notably, and research on the pathogenesis continues.2,
The incidence of KD in children under 5 years ranges from 3.4 to 218.6 cases per 100,000 children and varies regionally throughout the world. The prevalence of KD is highest in Asia, specifically in Japan, China, and Korea. Mortality associated with KD, which typically relates to cardiovascular complications, has been declining from greater than 1% in the 1970s to approximately 0.01% today. This decline in mortality is likely driven by trends toward earlier detection and increasing recognition of incomplete and atypical versions of the condition.5
UC is ideally suited for detection of KD, as the diagnosis relies heavily on clinical criteria. There are no laboratory findings specific to the diagnosis of KD. However, laboratory findings can offer support for the diagnosis and are required, especially in infants who less commonly have the major criteria present.
Case Presentation
A 3-year-old boy was brought in by his mother with concerns for 4 days of tactile fever, runny nose, and decreased appetite. The mother denied that the patient had any vomiting, diarrhea, cough, ear pain, rashes, recent travel, or insect bites. The patient’s vaccinations were up to date.
Vital signs at the initial visit included:
- Temperature: 39.7C
- Heart Rate: 154 beats per minute
- Blood Pressure: 90/60 mm/Hg
- Respiratory Rate: 24 breaths per minute, unlabored
- Oxygen Saturation: 99% (on room air)
Physical exam revealed the patient to be alert and in no distress. The patient’s eyes appeared watery, and there was mild conjunctival injection without purulent discharge. Bilateral tympanic membranes appeared normal. He had a strawberry-appearing tongue, erythema to the lips, and was drooling. There was mild bilateral, non-tender, anterior cervical lymphadenopathy (>1 cm). The patient’s cardiopulmonary and abdominal exams were unremarkable. There was a vague blanching maculopapular rash noted throughout the patient’s trunk and on the bilateral arms and legs, which spared the palms and soles.
During the visit, the patient had rapid swabs for Group A Streptococcus (GAS) and influenza, which were both negative, and a throat culture for Group A Streptococcus was sent to the lab, given consideration for scarlet fever. The patient was presumptively diagnosed with a viral infection.
The initial UC clinician recommended supportive treatment, prescribed saline nasal spray for congestion, and acetaminophen and ibuprofen as needed for fever. The mother was given strict return precautions including fever lasting more than an additional 2 or more days, or refractory to antipyretics, vomiting, difficulty breathing, rapid spreading of the rash, or other concerning changes.
Two days later, the throat culture results returned negative. The clinician following up on tests called the patient’s mother to inform her of the results; at that time, she stated that she was actually already on her way returning to the UC center because the fever had continued despite antipyretics. At this point, the patient had been febrile for a total of 6 days.
Vital signs at the second visit included:
- Temperature: 39.5C
- Heart Rate: 150 beats per minute
- Blood Pressure: 92/60 mm/Hg
- Respiratory Rate: 24 breaths per minute, unlabored
- Oxygen Saturation: 98% (on room air)
- Weight: 28 pounds (12.73 kilograms)
On physical exam, the patient seemed more fatigued than his initial visit but was non-toxic appearing. He was alert, but fussy, and had normal skin turgor. The patient had more pronounced conjunctival injection. It was noted that the erythematous rash on his trunk and extremities had increased since his first visit and now also involved the face. The mild, bilateral cervical lymphadenopathy was present and unchanged. The patient had moist mucous membranes and the strawberry tongue persisted and was now accompanied by pharyngeal erythema.
Differential Diagnosis and Medical Decision Making
KD is an important consideration to keep in mind whenever evaluating children with fever, however, certainly this is only one condition in a necessarily broad differential. Strep throat and other Group A Streptococcal infections (eg, scarlet fever) and influenza are common causes of pediatric fever. Thankfully, most UC centers have point-of-care (POC) testing available to evaluate for these conditions.
Adenovirus can mimic signs and symptoms of KD, especially when conjunctivitis and pharyngitis are present. However, adenovirus typically presents with exudative conjunctivitis, exudative pharyngitis, and fever, and typically does not present with other signs and symptoms of KD including erythema and swelling of the hands and feet, strawberry tongue, and rash. Some UC centers have access to respiratory viral panel (RVP) nucleic acid testing which may be considered in situations with an ambiguous etiology. However, clinicians should exercise caution in interpreting these tests as up to 70% of children presenting with fever may test positive for one or more viral pathogen, yet testing positive for a respiratory virus does not confirm this is the source of present fever.
POC urinalysis can be considered if urinary tract infections is suspected or when children present with fever and no localizing symptoms. In unvaccinated children, less common infections, such as measles, may be responsible. Depending on the geography and travel history, conditions ranging from leptospirosis to Rocky Mountain spotted fever (RMSF) might be considered. Finally, non-infectious causes such as Stevens-Johnson syndrome, hematologic malignancies, and autoimmune conditions, such as juvenile idiopathic arthritis, might be considered.
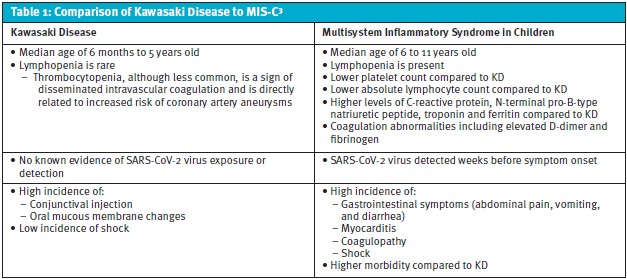
Kawasaki disease can mimic atypical pneumonia, with the possibility of interstitial and/or peribronchial infiltrates seen on chest radiography.7 In the presence of what seems like atypical pneumonia in children aged 3 and older, KD is a consideration when there is no response to antibiotics or the patient is failing to improve or defervesce as expected. This patient’s illness occurred before the COVID-19 pandemic. If he had been seen during the era of COVID, MIS-C secondary to COVID-19 certainly would have been important to include in the differential for this presentation. While almost half of the patients with MIS-C meet the criteria for KD, there are key differences between the two illnesses worth noting as detailed in Table 1.3
Final Diagnosis and Disposition
Given that this patient’s fever had lasted for 6 days and there were no alternate explanations for his symptoms, the clinician astutely had a high suspicion for KD. Although the patient did not meet all the major criteria for diagnosis, the UC clinician recommended that the patient be referred to the pediatric ED.
The pediatric clinicians caring for the patient diagnosed the patient with incomplete KD, and he was admitted and started on IVIG. He was hospitalized for nearly a week until the fevers had resolved and his echocardiogram was verified to be stable and normal. He subsequently followed up as an outpatient 1 month later in the pediatric cardiology clinic. A repeat echocardiogram did not show any coronary artery aneurysms, and the patient had fully recovered.
Discussion
KD is the leading cause of acquired coronary artery disease and heart disease in childhood. Treatment of KD with IVIG within 10 days of fever onset reduces the risk of these complications. Fortunately for the patient and his family, the clinician suspected KD on the sixth day of fever and referred him to the ED where the diagnosis was confirmed.
Laboratory tests that help in confirming the diagnosis of KD include elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), alanine aminotransferase, anemia, leukocytosis, hypoalbuminemia, and pyuria. Thrombocytosis commonly develops somewhat later in the disease course. Although these laboratory findings are not specific to KD, the diagnosis can be excluded if the platelet count, ESR, and CRP are normal after the seventh day of illness.
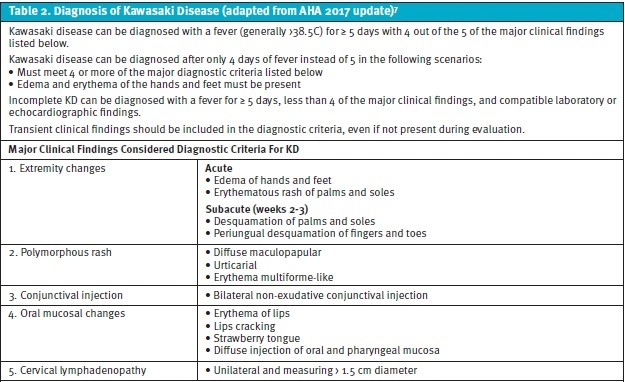
The diagnosis of KD relies on presence of clinical manifestations. The American Heart Association (AHA) first published the KD criteria for diagnosis in 2004, and these updated most recently in 2017.7 A high fever (at least 38.5-39C) must be present for 5 days or more and accompanied by 4 out of 5 of the major diagnostic criteria as seen in Table 2.7 If 4 or more of the major diagnostic criteria are met, and there is redness and swelling of the hand and feet, the diagnosis of KD can be made after only 4 days of fever instead of 5.7 Other diagnoses with similar symptoms importantly must be excluded to confirm KD, such as viral exanthems (eg, measles), other viral infections (eg, adenovirus and enterovirus), Stevens-Johnson syndrome, vector-borne illnesses (eg, RMSF), and GAS and Staphylococcal toxin-mediated diseases (eg, scarlet fever and toxic shock syndrome).10, It is important to note that not all criteria necessary to diagnose KD need be simultaneously present to make the diagnosis. To that end, when considering KD, it is worthwhile to inquire about the presence of symptoms that may have resolved prior to UC evaluation.
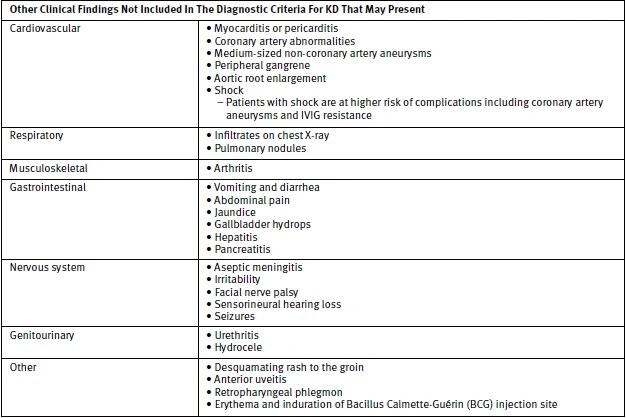
In addition to the major clinical findings, other signs and symptoms that may be present but are not diagnostic of KD are enumerated in Table 2.
KD tends to present with less overt symptomatology in infants. Diagnostic clues to KD in infants include the presence of prolonged fever and irritability, especially in those less than 6 months of age, or aseptic meningitis, culture-negative shock, cervical lymphadenitis unresponsive to antibiotics, and persistent pharyngeal inflammation unresponsive to antibiotics.7
If only 2 or 3 of the major clinical findings are met in addition to fever for at least 5 days, atypical, otherwise known as incomplete, KD may be diagnosed.14 Incomplete KD comprises between 15% and 35% of cases with the likelihood of incomplete, or atypical, KD being highest in children less than 12 months or over 5 years.4 Those with incomplete KD are roughly 3 times more likely to experience a delay in diagnosis.
The patient in this case report had incomplete KD as he only had 3 of the 5 major criteria present for diagnosis. Specifically, the major criteria present were: fever (>39C) for 6 days accompanied by a polymorphous rash, oral mucosal changes (ie, strawberry tongue and erythematous lips), and conjunctival injection. The patient had mild bilateral cervical lymphadenopathy, but it did not meet the specific criterion as they were not >1.5cm or unilateral.
The primary goal in the diagnosis of KD surrounds early identification, as this offers the best opportunity to prevent cardiac complications. IVIG and high-dose aspirin are the mainstays of treatment. The incidence of coronary artery aneurysms (CAA) is 15–25% in untreated patients, and less than 5% in patients who receive IVIG.4 CAA occur mostly in children less than 12 months and those older than 5 years, and in those for whom IVIG is initiated late in the disease process. Nearly 65% of children with KD under the age of 6 months will develop CAA, even if promptly treated with IVIG. It appears that the size of CAA is positively correlated with the duration of fever. If the fever lasts more than 10 days, it also increases the risk of IVIG resistance. Because of this, children with KD should start IVIG treatment within 10 days of fever onset to minimize cardiovascular morbidity and IVIG resistance.
Children with incomplete KD are at higher risk of developing CAA, which is largely felt to be attributed to delays in diagnosis. UC clinicians should consider this when discharging pediatric patients with suspected viral illnesses and ensure that parents seek repeat evaluation in the case of persistent fevers. It is also important to appreciate that KD can co-exist even in presence of infections if patients meet the diagnostic criteria for KD.7
Thankfully, the patient outlined had a favorable outcome, as do most children when KD is diagnosed early and appropriate treatment is initiated. Unfortunately, patients who are not diagnosed with KD in a timely fashion, as is often the case with incomplete KD, may not respond to standard therapies and are at higher risk of serious cardiac complications.
Take Home Points
Kawasaki disease is a clinical diagnosis. Lab tests can be helpful but do not confirm the diagnosis of KD.
- To diagnose KD, a high fever (>38.5C) must be present for at least 5 days and accompanied by a minimum of 4 out of the 5 the major criteria which are:
- Extremity changes, including erythematous rash and swelling of palms and soles
- Polymorphous rash
- Conjunctival injection
- Oral mucosal changes
- Unilateral cervical lymphadenopathy
- If there are 4 or more of the major diagnostic criteria met, and there is redness and swelling of the hand and feet, the diagnosis of KD can be made after only 4 days of fever.
- If only 2 or 3 of the major diagnostic criteria are met with at least 5 days of fever incomplete KD may be diagnosed.
- The symptoms of KD do not have to be present at the same time to make the diagnosis. It is important to ask parents about the presence of symptoms that may have been resolved before the urgent care visit.
- The primary goal is to diagnose KD as early in the disease process as possible to avoid the complications associated with it, including coronary artery aneurysms, or coronary artery dilatation, and IVIG resistance.
- IVIG is the mainstay of treatment, along with high-dose aspirin for anti-inflammation.
- Strict return precautions are important to convey to parents, especially when there is suspicion for KD.
Ethics Statement and Patient Perspective
The patient and his family were lost to follow-up and were therefore unable to give consent. Patient demographics were changed to protect patient anonymity and confidentiality.
Manuscript submitted August 3, 2023; accepted January 10, 2024.
References
- Kawasaki T. Kawasaki disease. Int J Rheum Dis. 2014;17(5):597-600. doi:10.1111/1756-185X.12408
- Sakurai Y. Autoimmune Aspects of Kawasaki disease. J Investig Allergol Clin Immunol. 2019;29(4):251-261. doi:10.18176/jiaci.0300
- Sharma C, Ganigara M, Galeotti C, et al. Multisystem inflammatory syndrome in children and Kawasaki disease: a critical comparison. Nat Rev Rheumatol. 2021;17(12):731-748. doi:10.1038/s41584-021-00709-9
- Lee JK. Hygiene Hypothesis as the Etiology of Kawasaki disease: Dysregulation of early B cell development. Int J Mol Sci. 2021;22(22):12334. doi:10.3390/ijms222212334
- Marchesi A, Tarissi de Jacobis I, Rigante D, et al. Kawasaki disease: guidelines of the Italian Society of Pediatrics, part I – definition, epidemiology, etiopathogenesis, clinical expression and management of the acute phase. Ital J Pediatr. 2018;44(1):102. doi:10.1186/s13052-018-0536-3
- Wilder MS, Palinkas LA, Kao AS, Bastian JF, Turner CL, Burns JC. Delayed diagnosis by physicians contributes to the development of coronary artery aneurysms in children with Kawasaki syndrome. Pediatr Infect Dis J. 2007;26(3):256-260. doi:10.1097/01.inf.0000256783.57041.66
- McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135(17). doi:10.1161/CIR.0000000000000484
- Fortenberry M, Zummer J, Maul E, Schadler A, Cummins M, Pauw E, Peta N, Gardner B. Use and Cost Analysis of Comprehensive Respiratory Panel Testing in a Pediatric Emergency Department. Pediatr Emerg Care. 2023 Mar 1;39(3):154-158. doi: 10.1097/PEC.0000000000002695. Epub 2022 Apr 12. PMID: 35413042.
- Dayal R, Agarwal D. Fever in Children and Fever of Unknown Origin. Indian J Pediatr. 2016 Jan;83(1):38-43. doi: 10.1007/s12098-015-1724-4. Epub 2015 Mar 1. PMID: 25724501.
- Singh S, Jindal AK, Pilania RK. Diagnosis of Kawasaki disease. Int J Rheum Dis. 2018;21(1):36-44. doi:10.1111/1756-185X.13224
- Hedrich CM, Schnabel A, Hospach T. Kawasaki Disease. Front Pediatr. 2018;6:198. doi:10.3389/fped.2018.00198
- Lee W, Cheah CS, Suhaini SA, Azidin AH, Khoo MS, Ismail NAS, Ali A. Clinical Manifestations and Laboratory Findings of Kawasaki Disease: Beyond the Classic Diagnostic Features. Medicina (Kaunas). 2022 May 30;58(6):734. doi: 10.3390/medicina58060734. PMID: 35743997; PMCID: PMC9227912.
- Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Pediatrics. 2004;114(6):1708-1733. doi:10.1542/peds.2004-2182
- Rife E, Gedalia A. Kawasaki Disease: an update. Curr Rheumatol Rep. 2020;22(10):75. doi:10.1007/s11926-020-00941-4
- Mat Bah MN, Alias EY, Sapian MH, Abdullah N. Delayed diagnosis of Kawasaki disease in Malaysia: Who is at risk and what is the outcome. Pediatr Int. 2022;64(1):e15162. doi:10.1111/ped.15162
- Van Stijn D, Korbee JM, Netea SA, et al. Treatment and coronary artery aneurysm formation in Kawasaki disease: A per-day risk analysis. J Pediatr. 2022;243:167-172.e1. doi:10.1016/j.jpeds.2021.12.054
- Berdej-Szczot E, Małecka-Tendera E, Gawlik T, Firek-Pędras M, Szydłowski L, Gawlik A. Risk factors of immunoglobulin resistance and coronary complications in children with Kawasaki disease. Kardiol Pol. 2017;75(3):261-266. doi:10.5603/KP.a2016.0179
- Mossberg M, Mohammad AJ, Kahn F, Segelmark M, Kahn R. High risk of coronary artery aneurysm in Kawasaki disease. Rheumatology. 2021;60(4):1910-1914. doi:10.1093/rheumatology/keaa512
Author Affiliation: Dominic K. Hardatt, DMSc, PA-C, Northwell Health, GoHealth Urgent Care. The author has no relevant financial relationships with any ineligible companies.
Click Here to download the article PDF
Read Similar Articles
- Is It Measles Or Something Else?
- Management Of Erythema Multiforme In The Urgent Care Setting
- Multisystem Inflammatory Syndrome In Children (MIS-C): Who Should Not Be MISC’ed?