Published on
Urgent message: Back pain is a common complaint in the urgent care setting. Common causes of musculoskeletal back pain include overuse and work-related injury. Other causes can include disc herniation, metastasis, osteoporosis, arthritis, spinal stenosis, and nephrolithiasis.
Crystal N. Bharat MD, Ronald Dvorkin, MD, and Glenn G. Gray MD
Case Presentation
A 65-year-old female complained of 1 day of low back pain radiating to her left flank, which was aggravated with movement. Symptoms began while at work. Patient denied nausea, vomiting, diarrhea, fever, urinary frequency, urinary urgency, dysuria and hematuria, bowel or bladder dysfunction, or lower-extremity or gluteal paresthesias. On her physical exam, paravertebral muscle spasm was appreciated with mild midline tenderness and no mass.
Neurological sensation was intact. Motor strength was 5/5 and reflexes 2+ in the lower extremities bilaterally. Lumbar radiographs were negative, without acute findings. Patient was diagnosed with lumbar strain and treated with cyclobenzaprine (Flexeril) and naproxen sodium (Naprosyn).
The patient returned the following day due to her inability to perform normal work activities. She complained of left flank pain radiating to her left abdominal region. Abdominal and flank palpation elicited mild left lower quadrant tenderness. Urinalysis did not show evidence of blood or infection. A CT of the abdomen and pelvis without contrast was ordered to evaluate for a ureteral stone, diverticulitis, or incarcerated hernia. Radiology reported an incidental left posterior flank soft tissue lipoma; the scan was otherwise unremarkable. Patient was advised to continue with current medication, rest, and return in 2 days for reevaluation.
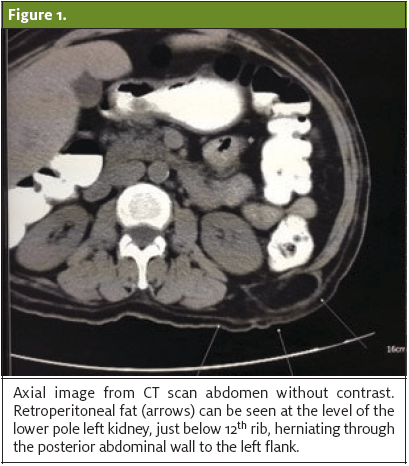
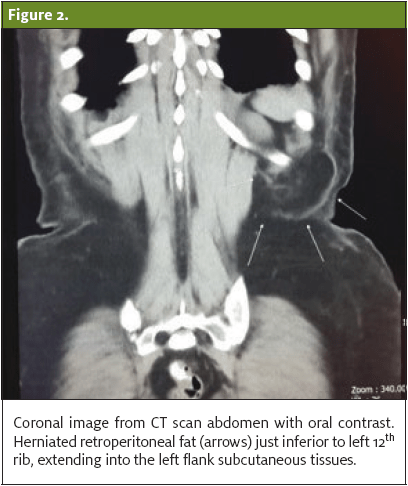
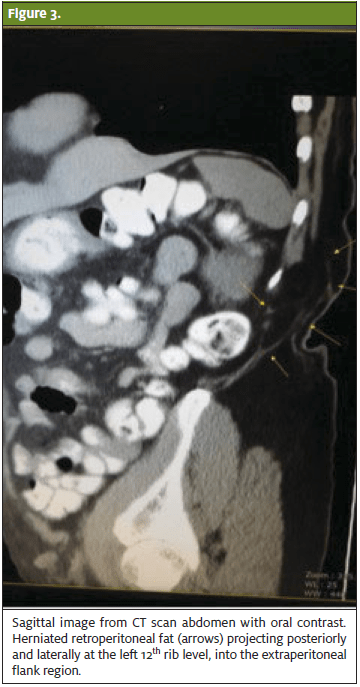
Upon the third visit, the patient reported persistent left flank pain with radiation to the left inguinal region. Repeat urinalysis was within normal limits. A radiologist was called to discuss and review previous CT scan of the abdomen and pelvis. Upon further review, it was noted that the previously described left flank fatty lesion was herniated fat posterior to the left kidney which progressed through the superior lumbar triangle. (See Figures 1–3.)
Discharge Instructions
Patient was advised to follow up with general surgery.
Discussion
The differential diagnosis of low back pain is broad. Though older adults can experience pain related to any condition affecting younger adults, patients over 60 years of age are more likely to have pain related to degeneration of the spinal joint, including osteoporosis and spinal stenosis. Consideration should also be made for neoplasm, infection, and abdominal aortic aneurysm.
Red flags for serious causes of back pain include fever, weight loss, numbness, history of malignancy, nighttime pain, and urinary retention or incontinence. Chronic undifferentiated low back pain (>6 weeks) may also deserve additional work-up.
A lumbar hernia is a rare entity, with <300 cases reported in the literature.1 Symptoms can vary and may be difficult to distinguish between other etiologies. Palpation of both superior and inferior triangles may confirm an important clinical finding, a bulge.2 However, a palpable mass or bulge in the lumbar area does not need to be appreciated, as seen in our case. The ability to diagnose a lumbar hernia during the initial patient visit may be challenging without further diagnostic testing, such as a CT scan.
The superior lumbar triangle is bordered by the 12th rib superiorly, iliac crest inferiorly, erector spinae muscle medially, and posterior oblique muscle laterally.3 There are two types of hernias that are determined by their anatomical location—the superior lumbar hernia (Grynfeltt-Lessshaft hernia), as in this case, and the inferior lumbar hernia (Petit hernia). If initial treatment fails and clinical symptoms do not correlate with radiological exam, it is important to reevaluate past diagnostic imaging and question initial radiology reports.
The most effective treatment approach is best determined by properly identifying classification, size, location, and contents of defect with CT imaging, which allows surgeons to choose which method (open vs laparoscopic) to perform.4 Surgical repair with synthetic mesh has been found to be successful with minor complications and tissue damage.5
Conclusion
Since lumbar hernias are rare, diagnosis may often be made retrospectively. In this case, the symptoms were not consistent with the initial radiological interpretation. When clinical suspicion is discordant with an imaging study, direct consultation with a radiologist can often help in establishing an unusual diagnosis.
Citation: Bharat CN, Dvorkin R, Gray GG. Lumbar hernia: an unusual cause of back pain. J Urgent Care Med. November 2017. Available at: https://www.jucm.com/lumbar-hernia-unusual-cause-back-pain/.
References
- Mingolla GP, Amelio G. Lumbar hernia misdiagnosed as subcutaneous lipoma: a case report. J Med Case Rep. 2009;3:9322.
- Lillie GR, Deppert E. Inferior lumbar triangle hernia as a rarely reported cause of low back pain: a report of 4 cases. J Chiropr Med. 2010:9(2):73-76.
- Hide IG, Pike EE, Uberoi R. Lumbar hernia: a rare cause of large bowel obstruction.Postgrad Med J. 1999;75(882):231–232.
- Moreno-Egea A, Baena EG, Calle MC, et al. Controversies in the current management of lumbar hernias. Arch Surg.2007;142(1):82-88.
- Mismar A, Al-Ardah M, Albsoul N, Younes N. Underlay mesh repair for spontaneous lumbar repair. Int J Surg Case Rep. 2013;4(6):534-536.

Crystal N. Bharat, MD

Glenn G. Gray, MD
