
Urgent message: Triage of eye conditions in urgent care to ensure the best patient outcome requires knowing what equipment to use and understanding when to refer to an ophthalmologist. Always remember to document acuity of vision in all patients presenting with an eye complaint.
SARVOTHAM KINI, MD
Introduction
Ocular complaints are extremely common in the urgent care setting. Yet the capacity of individual urgent care centers to provide high quality eye care is variable. The equipment available and the proficiency of the clinician are equally important factors. This article intends to more clearly define the scope of acute eye care and its prevalence in the urgent care setting, while identifying the equipment and decision-making guidance necessary for high-quality and best outcomes. Understanding when to solicit the expertise of an ophthalmologist and appre ciating the appropriate timing of these referrals is covered for each of the commonly encountered eye conditions discussed here. It is of utmost importance to distinguish sight-threatening from routine eye conditions to ensure appropriate rapid referral decisions. Most other acute eye conditions can be managed in the urgent care setting with basic eye care tools and best-practice management principles.
Tables 1 and 2 create the framework for this two part series by identifying the most common eye complaints and the sight threatening conditions not to be missed in your evaluation of each. In Part 1, we will discuss foreign bodies, corneal abrasion, red eye, scleritis, and conjunctivitis. Part 2, in a subsequent issue, will review subconjunctival hemorrhage, uveitis, iritis, keratitis, acute angle closure glaucoma, and eyelid conditions.
| Table 1. Common Ocular Complaints | |
|
|
| Table 2. Vision-Threatening Conditions | |
|
|
| Table 3. Indications for slit-lamp examination |
|
Initial Evaluation
Serious eye conditions such as ocular trauma, complex eyelid lacerations, chemical burns and acute vision loss are only rarely encountered in urgent care. Patients with these conditions should be referred urgently to the nearest emergency department or to an ophthalmologist.
As with other urgent care presentations, evaluation of eye complaints should start with a good history and review of systems. Assessment of visual acuity is paramount to the eye evaluation and should be obtained with corrective lenses whenever possible. For patients who forget to bring their glasses to the visit, use of the “Pin Hole” technique (back of a prescription pad with a few holes created by using an 18G needle) reproduces optically corrected vision in most cases.
While the exam is focused primarily on the eyes, evaluation of the surrounding skin, head and neck may reveal clues to non-ocular causes of eye symptoms. For example, a papulo-vesicular scalp rash associated with “red eye” and pain is an important clue for herpes zoster ophthalmicus. In addition, a focused neurologic exam can reveal important clues to the diagnosis and may identify more concerning central nervous system pathology. Examples are multiple sclerosis, myasthenia gravis and cranial nerve palsies. Not every patient with an eye complaint needs a slit lamp examination.1 Slit lamp does, however, provide many valuable findings, if one is comfortable using it. It is especially useful under the conditions listed in Table 3. Good training in how to use a slit lamp properly will be necessary.
Fluorescein staining should be a routine part of any eye exam when evaluating red eye, eye trauma, foreign bodies or contact lens irritation. Fluorescein is contraindicated in hyphema, chronic inflammation, most chemical exposures and for patients with high-velocity injuries.
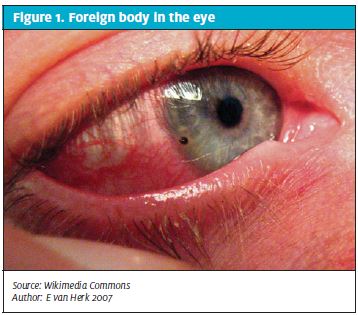
Foreign bodies in the eye
If a patient complains of a sensation of a foreign body in the eye under the lid, resist the temptation to administer local anesthetic drops because the numbing will prevent the patient from confirming that the discomfort has abated when the particle is removed. Start by offering comfort and then search for the foreign body under the eyelid (Figure 1) or over the surface of the cornea. Flip the patient’s eyelid and, if you find a particle, wipe it off with a wet cotton swab. If, after the particle is removed, the patient confirms that the original sensation is gone, then he or she can be discharged home.
If you are unable to locate the particle, proceed with instilling a few drops of tetracaine or pontocaine in the affected eye. Then stain the eye with fluorescein and examine the cornea. Corneal abrasions that are linear suggest a foreign body under the lid and a need to search further. Sometimes abrasions are a residual finding from a particle scratching the cornea that was not found and may have washed off, leaving the patient with the sensation of a foreign body.
Fluorescein strips are considerably more hygienic than drops from a bottle and they limit the amount of dye that gets into a patient’s eye. Instillation of fluorescein drops to the point of overflowing can lead to difficulty distinguishing between excess dye from an aqueous leak versus fluid from a potential globe rupture.
Urgent care providers occasionally see patients who have a metallic foreign body on the cornea. This presentation can occur when a patient’s occupation involves striking metal to metal and a small metal particle flies into the eye. A cotton-tipped swab is a good initial tool to remove such particles. If removal with a swab is not successful, the tip of a 25G hypodermic needle can be used to scrape the particle gently and carefully. Even after a metal particle is successfully removed, a residual rust ring may remain on the cornea. An ophthalmic “burr” can be used to remove this rust ring or the patient can be referred to an ophthalmologist.
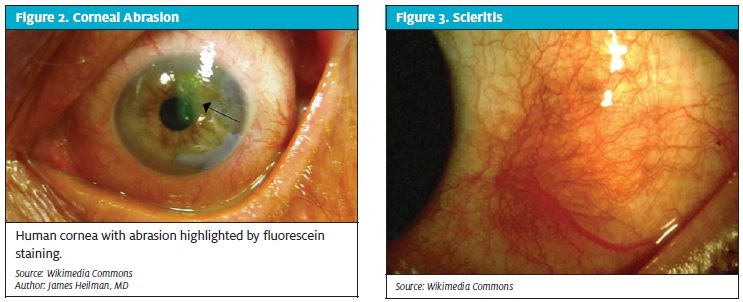
Corneal Abrasion
Corneal abrasions can be small and superficial (Figure 2) or large and deep.2 They are typically painful and associated with excessive tearing and they can be associated with redness and complaints of photophobia. A fluorescein strip and a Woods lamp are all that is needed to diagnose an isolated corneal abrasion. Slit lamp examination may show some flares and floaters in the anterior chamber secondary to iritis, especially if there was a delay in getting medical help. The treatment for small and superficial abrasion is comfort measures and dark glasses. An eye patch is unnecessary and may even cause more discomfort and delay a patient’s healing. Most superficial abrasions heal within 2 to 3 days. Larger abrasions can be patched for the sake of patient comfort, but close patient follow up or referral to an ophthalmologist is necessary in those cases.
Red eye
Most patients with a red eye will assume it is a bacterial infection and ask for an antibiotic. Eye redness can be due to many causes, including a bacterial infection, but the most common cause of red eye is viral infection, usually due to adenovirus.3,4 It may be difficult to distinguish between viral and bacterial infection of the eye. A thorough history and exam may reveal clues.
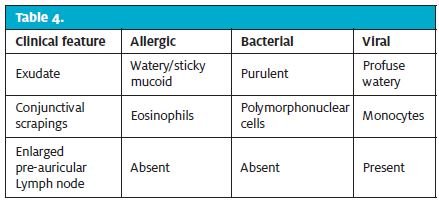
Matting of the eyes on waking is not definitive evidence of a bacterial infection. The most common symptoms of any conjunctivitis are redness; foreign body (sand-like) sensation; excessive tearing, pain and discomfort; and discharge. On initial examination, determine the degree of redness over the globe of the eye and inside the eyelid (palpebral conjunctiva). If the palpebral conjunctiva is redder than the bulbar conjunctiva, the diagnosis is conjunctivitis. If the bulbar conjunctiva is redder than the palpebral conjunctiva, the diagnosis of a more serious condition, such as scleritis (Figure 3), iritis, iridocyclitis or acute angle closure glaucoma should be considered.
Occasionally patients present with a localized patch of redness from a group of injected blood vessels on the sclera (episcleritis) or a dark red, painless collection of blood under the conjunctiva (subconjunctival hemorrhage). These are very different and rather benign clinical entities.
Table 4 lists the three most important causes of conjunctivitis and their distinguishing features.
Allergic conjunctivitis
Allergic conjunctivitis (Figure 4) is a benign inflammation of the conjunctiva that is common in young adults. It is caused by environmental exposure and does not affect vision. Patients with allergic conjunctivitis often have a history of other allergic conditions such as hay fever, asthma, and atopic dermatitis. The presentation is tearing, eye redness and significant itching. Patients may tend to downplay their itching whereas family members may notice that they rub their eyes constantly, which is a giveaway. Symptoms are usually bilateral but one eye may be worse than the other.
Allergic conjunctivitis is primarily a clinical diagnosis. Advanced testing is not usually indicated. Presence of eosinophils and mast cells in conjunctival scrapings under the microscope will help establish a diagnosis of allergic conjunctivitis. Secondary infections and corneal abrasions (due to rubbing of eyes) are relatively common complications. A sudden acute worsening, change in mucus from clear to purulent, or eye pain (secondary to abrasion), are clues to the development of these complications.
Treatment of allergic conjunctivitis consists of frequent use of artificial tears to help wash out the allergens.5,6 Topical antihistamines and mast cell stabilizers (Zaditor drops, or Olopatadine (brand name Patanol) will relieve the symptoms rapidly. Application of cold compresses hastens the resolution of symptoms. Advising patients to avoid exposure to known allergens is important. Patients should also be counseled to avoid wearing contact lenses until their symptoms have completely abated. Nasal corticosteroids and oral antihistamines are commonly prescribed concurrently to improve response.
Bacterial Conjunctivitis
Organisms that commonly cause acute bacterial conjunctivitis (Figure 5) are Staphylococcus aureus (common in adults), Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis, which are common in children.7-9
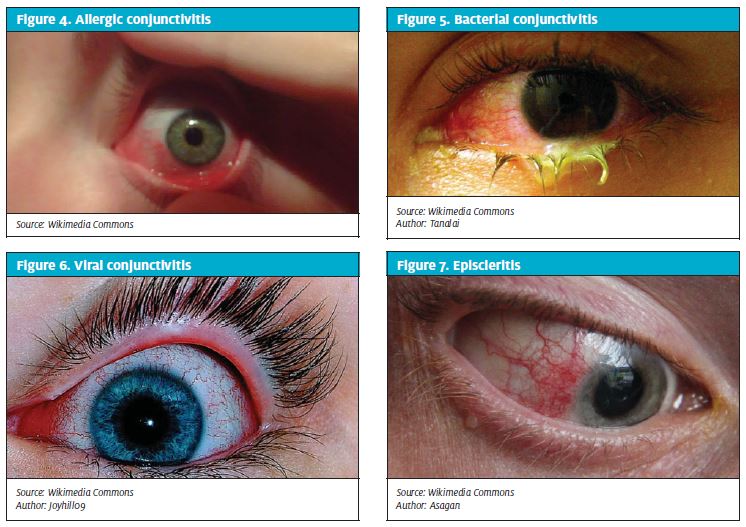
Bacterial conjunctivitis can be unilateral or bilateral and is highly contagious. Common symptoms are redness and discharge, which can be white, yellow or green. The eyelids can be swollen and stuck together, especially in the mornings, a feature that is not generally useful in distinguishing the various types of conjunctivitis. The eyelids may be tender to palpation. Definitive diagnosis of bacterial conjunctivitis is established from cultures obtained from the conjunctival sac.
Conjunctivitis can also be caused by Neisseria species, particularly N. gonorrhea, which is more serious and carries threat to vision. This infection needs to be treated aggressively with intravenous antibiotics and an ophthalmology consult is recommended.
Common ophthalmic antibiotics that are useful for treatment of acute conjunctivitis are sulfacetamide 10% drops, erythromycin ophthalmic ointment, tobramycin drops, and polymyxin B/trimethoprim drops. Each of these therapeutic options has its problems. Sulfacetamide burns, ointment preparations are messy, polymyxin and tobramycin can be sensitizing and along with allergies to any of the components, can produce the appearance of worsening infection when sensitization is the underlying cause. Do not patch an eye affected by acute conjunctivitis. The best comfort measure, particularly outdoors, is wearing dark glasses.
Viral Conjunctivitis
Adenovirus is the major cause of viral conjunctivitis (Figure 6).10 It is highly contagious and can remain so for up to 10 days. Patients should be warned about this virus and instructed to wash their hands before and after using drops and even touching their eyes. Treatment generally consists of comfort measures such as cool compresses, artificial tears, and dark glasses in the bright sun. Antibiotics do not help and should not be prescribed. Patient education goes a long way in management of this infection.
One form of viral conjunctivitis, epidemic keratoconjunctivitis (EKC), is particularly fulminant. It can involve the cornea and thus affect the vision. Keratitis is potentially vision-threatening and these patients should be referred to an ophthalmologist.
Scleritis
Scleritis (Figure 3) is uncommon, but often occurs with systemic disorders, specifically autoimmune diseases and infections. Scleritis is inflammation of the tenon capsule and patients with it present with dull boring pain and tenderness over the globe of the eye. Diffuse injection of the blood vessels gives a dark red or purple color to the globe and photophobia and poor vision are common. Patients with suspected scleritis need further work up for rheumatologic disorders such as rheumatoid arthritis, Wegener’s granulomatosis, seronegative spondyloarthropathies, relapsing polychondritis, and systemic lupus erythematosus. Tuberculosis, syphilis and sarcoidosis are also known to cause scleritis. Other causes of painful red eye such as iritis, keratitis, and acute angle closure glaucoma should be considered as well.
Scleritis is initially treated with systemic nonsteroidal anti-inflammatory drugs (NSAIDs) and/or topical steroids. Two drops of 1% prednisolone every 2 hours for up to 2 weeks can be tried, initially, while a patient waits to be seen by a rheumatologist or ophthalmologist. Other treatments such as systemic steroids, subconjunctival steroids, and immune modulators may need to be considered by a rheumatologist and or an ophthalmologist.
Episcleritis
Episcleritis (Figure 7) is most often idiopathic, but may also be associated with any of the rheumatologic diseases that cause scleritis. Episcleritis is typically benign, often segmental, but can be diffuse. Examination of the eye shows an inflamed group of conjunctival blood vessels over a segment of the globe. There may be some tenderness over the area of inflammation. Episcleritis does not cause visual loss and often resolves spontaneously. In these patients, eye redness and irritation improve by 50% in less than a week. Treatment with topical NSAIDs and/or artificial tears will resolve the redness and discomfort.
Conclusion
Eye conditions and complaints are extremely common in the urgent care setting. The ability to carefully evaluate and triage these conditions is essential to favorable outcomes. Through the use of readily accessible tools and prudent referrals, most eye problems can be initially managed in the urgent care setting. Understanding the nature and course of sight-threatening complications and the diagnostic clues that identify them helps guide the clinician through safe and effective decision-making for patients with acute eye conditions.
References
- Babineau MR et al. Ophthalmologic procedures in the emergency department. Emerg Med Clin North Am. 2008 Feb;26(1):17–34. [PMID: 18249255]
- Goh PP et al. Contact lens—related corneal ulcer: a two-year review. Med J Malaysia. 2010 Jun;65(Suppl A):120–3. [PMID: 21488471]
- Cronau H et al. Diagnosis and management of red eye in primary care. Am Fam Physician. 2010 Jan 15;81(2):137–44. [PMID: 20082509]
- Powdrill S. Ciliary injection: a differential diagnosis for the patient with acute red eye. JAAPA. 2010 Dec;23(12):50–4. [PMID: 21229837]
- Bielory BP et al. Management of seasonal allergic conjunctivitis: guide to therapy. Acta Ophthalmol. 2012 Aug;90(5):399–407. [PMID: 22067457]
- Bielory L. Allergic conjunctivitis: the evolution of therapeutic options. Allergy Asthma Proc. 2012 Mar–Apr;33(2):129–39. [PMID: 22525389]
- Drug and Therapeutics Bulletin. Management of acute infective conjunctivitis. Drug Ther Bull. 2011 Jul;49(7):78–81. [PMID: 21733975]
- Epling J. Bacterial conjunctivitis. Clin Evid (Online). 2012 Feb 20;2012. [PMID: 22348418]
- Hutnik C et al. Bacterial conjunctivitis. Clin Ophthalmol. 2010 Dec 6;4:1451–7. [PMID: 21188158]
- Skevaki CL et al. Treatment of viral conjunctivitis with antiviral drugs. Drugs. 2011 Feb 12;71(3):331–47. [PMID: 21319870]