
Urgent message: Whether benign or vision-threatening, acute eye conditions seen in the urgent care setting require careful evaluation and triage, based on access to the right tools and knowledge of key clues to diagnosis.
SARVOTHAM KINI, MD
In Part 1 of this article in January, we discussed urgent care management of foreign bodies in the eye, corneal abrasion, red eye, scleritis, and conjunctivitis. In Part 2, we will review subconjunctival hemorrhage, uveitis, iritis, keratitis, acute angle closure glaucoma, and eyelid conditions.
Subconjunctival hemorrhage
Trivial events such as a cough, sneeze, Valsalva maneuver, or minor blunt trauma can cause bleeding under the conjunctiva. Patients with subconjunctival hemorrhage (Figure 1) may present with some degree of discomfort and anxiety secondary to the appearance of the bloody eye. The blood is usually bright red, appears flat, and is limited to the bulbar conjunctiva and stops abruptly at the limbus. It is important to differentiate the lesion from bloody chemosis, which can occur with globe rupture. Aside from appearance, this condition does not cause patients any pain or diminution in visual acuity.
Patients with subconjunctival hemorrhage should be warned about any excessive NSAID use and also reassured that complete resolution of their condition may take up to 3 weeks.

Iritis
Uveitis is an inflammation of the uveal tract that includes iritis of unknown origin and can be secondary to trauma or other nontraumatic conditions such as rheumatoid arthritis and inflammatory bowel disease.1-5 Iritis (Figure 2), arthritis, and urethritis are aspects of Reiter’s syndrome.
Iritis can occur at any age but is most common in patients aged 20 to 59 years.
Injection, photophobia, pain, and blurred vision are the common symptoms of iritis (anterior uveitis or iridocyclitis). The diagnosis is made with these clinical symptoms and a slit lamp examination. Leukocytes and fibrous debris in the anterior chamber along with intense ciliary flush are seen under the slit lamp.
Treatment with a topical corticosteroid and a cycloplegic agent is recommended to relieve the inflammation and prevent complications such as cataract and glaucoma. With a preliminary diagnosis of iritis, or any other significant, non-infectious, inflammatory condition, urgent care treatment with a corticosteroid is reasonable as long as ophthalmology follow-up can be assured. Extended treatment with topical corticosteroids is discouraged without ophthalmology consultation. Ophthalmology referral for iritis is recommended.
Keratitis
Keratitis (Figure 3) is inflammation of the cornea that can be due to infectious or non-infectious causes.6-9 Bacteria, viruses, fungi, and spirochetes can affect the cornea and destroy the corneal epithelium, leading to corneal ulcer in severe cases. Important causes of keratitis to remember are Herpes simplex virus (HSV), HSV-I and HSV- II, Herpes zoster and pseudomonas. HSV presents as typical dendritic ulcer on the surface of the cornea, which can be detected with fluorescein with or without slit lamp examination. Herpes zoster affects the ophthalmic branch of the trigeminal nerve and may produce a rash on the forehead and affect the cornea, both of which are painful and need to be treated aggressively.
Keratitis is a threat to vision because of the risk of corneal clouding, scarring, and perforation. Trachoma from chlamydial infection is a leading cause of blindness in the third world. In the United States, contact lenses play a major role in corneal infection and ulceration.
Patients with keratitis and corneal ulcer present with pain, eye discharge, photophobia and poor vision. A “white spot” on the cornea with these symptoms is due to a corneal ulcer until proved otherwise. Patients who wear “extended-wear” contact lenses and neglect to remove them at night have a 20-fold higher risk of developing corneal ulcer compared to those who are conscientious about the use of their lenses.6
Slit-lamp examination shows disruption of the corneal epithelium, an infiltrate in the corneal stroma, and even purulent collection (hypopion) in the anterior chamber.

Although immediate empirical antibiotic therapy is recommended for keratitis, it is important to obtain corneal scrapings for Gram’s stain, Giemsa stain, and cultures. Thus, treatment in direct consultation with an ophthalmologist is advised. Ciprofloxin ophthalmic drops are a recommended treatment for pseudomonas infection of the cornea.
Herpes simplex keratitis is treated with topical antiviral agents, cycloplegics, and oral acyclovir. Steroids are generally not recommended in treatment of Herpes Simplex I, because of the risk of corneal melting and perforation.10
Herpes zoster is easier to diagnose when the rash is in the typical dermatomal distribution over the eye. Hutchinson’s sign is a rash over the tip of the nose, caused when the virus affects the nasociliary branch of the ophthalmic nerve, and a strong indication that the cornea is affected. Often the patient presents prior to the onset of rash, making diagnosis challenging. Given the significant risk associated with this condition, any patient with signs or symptoms of facial nerve pain and eye redness should be treated empirically for herpes keratitis until ophthalmology follow-up.
Herpes zoster ophthalmicus is treated with antiviral agents and cycloplegics. In severe cases, topical steroids can be added to prevent corneal scarring potentially leading to blindness.
Ultraviolet keratitis is an interesting clinical entity that you may be asked to see in an urgent care setting. Some patients develop ultraviolet keratitis after use of a sunlamp without eye protection, exposure to a welding arc, or exposure to the sun when skiing (“snow blindness”).
Symptoms typically develop 8 to 12 hours post exposure and consist of severe bilateral eye pain with excessive watering and photophobia. The diagnosis can be made with use of fluorescein drops and examination under the slit lamp. Diffuse punctate staining of the cornea is confirmatory.
Ultraviolet keratitis is treated with instillation of 1 to 2 drops of Cyclogyl (to relieve ciliary spasm) and patching of both eyes. All patients recover within 24 to 48 hours without complications. Local anesthetics tend to delay corneal epithelial healing, hence prescribing local anesthetic drops for outpatient use must be discouraged.11,12
Acute angle closure glaucoma
Acute angle closure glaucoma (Figure 4) is a rare and frequently misdiagnosed cause of a red, painful eye. When a patient presents with a painful red eye that is “rock hard’ to digital palpation of the globe with or without corneal clouding, acute angle closure glaucoma should be considered and intraocular pressure should be measured in both eyes.13-16 A tonopen is a handy tool for measuring intraocular pressure that should be available to urgent care providers. Normal pressure is less than 20 mm of Hg.17
Headache, nausea and blurred vision are common associated symptoms in patients with high intraocular pressure. Urgent care physicians can use a simple yet reliable tool, tonopen to measure the intraocular pressure.17 Initial treatment of the condition includes topical betablockers, prostaglandin analogues, _2-adrenergic agonists, and pilocarpine to induce meiosis. Induction of meiosis opens up the angle and improves aqueous humor flow, thus reducing intraocular pressure. If the intraocular pressure is extremely high, the cornea will appear cloudy and the pupil will be mid-dilated and non-reactive to light. In that case, oral or intravenous acetazolamide may need to be used to improve the pressure, only after which will the topical drops begin to work.
Ophthalmology referral for acute angle closure glaucoma is crucial for definitive treatment (peripheral iridectomy) in a timely fashion to improve symptoms, lower the intraocular pressure, and save vision.
Lid conditions
Stye (Figure 5) or hordeolum is a common staphylococcal infection of the glands of Zeiss that can present as an abscess on the outside on the lid margin or inside on the palpebral conjunctiva.18 Characteristic features are localized redness, swelling, and an acutely tender area on the upper or lower lid. Warm compresses are helpful and may resolve the symptoms at an early stage. Antibiotic ointment (bacitracin or erythromycin) applied to the eyelid every 3 hours may be beneficial during the acute stage. Incision is rarely indicated if a small pinpoint pustule progresses to form an abscess.

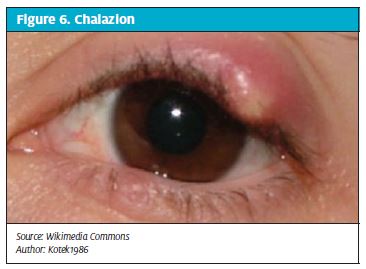
A chalazion (Figure 6) is a common granulomatous inflammation of a meibomian gland of the eyelid.19 Patients with a chalazion present with a hard, nodular swelling on the upper or lower lid with or without redness and swelling of the adjacent conjunctiva. Chalazia can get infected. Treatment is usually with warm compresses, gentle massage and incision, and curettage20 from the conjunctival surface of the lid, but corticosteroid injection may also be effective for chronic chalazia. At times, patients seek medical advice for chalazia, for cosmetic reasons.
Blepharitis
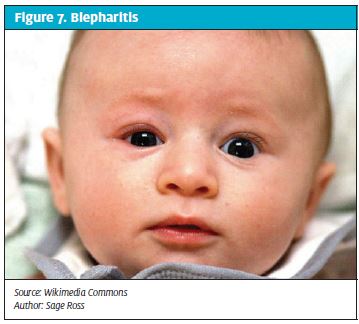
Blepharitis (Figure 7) is a common bilateral staphylo coccal infection of the Meibomian, Zeis and Moll glands in the eyelid margins.21-22 Blepharitis can be associated with seborrhea of the scalp, eyebrows, and ears and its severity and time course may vary.
Patients with blepheritis complain of eyelid irritation, burning, and itching. The eyes are red over the lid margins and the immediate surrounding area of skin shows scales or granulation. Flakes can be seen clinging to the lashes.
Treatment involves warm wet compresses and lid hygiene consisting of washing with baby shampoo and removing the scales (lid margin debris). Associated seborrhea should be controlled as well.
Anti-staphylococcal antibiotic eye ointment such as bacitracin or erythromycin is rubbed daily on the lid margins, during acute exacerbations. At times blepharitis can exist along with a stye or chalazion.
Dacryocystitis
Acute or chronic dacryocystitis is infection of the lacrimal sac secondary to obstruction of the nasolacrimal system.23 It occurs most often in infants and in individuals older than age 40 years. It is usually unilateral.24
- aureus and beta-hemolytic streptococci cause acute dacryocystitis. Staphylococcus epidermidis, anaerobic streptococci, and Candida albicans can cause chronic dacryocystitis.
Patients with dacryocystitis present with pain, swelling, tenderness, and redness over the tear sac area near the medial canthus of the eye. Purulent material may be expressed through the tear duct. Chronic dacryocystitis can present with tearing and mucous or purulent discharge. Older patients may develop small stones in the lacrimal sac (dacryoliths), which may precipitate the infection.
Acute dacryocystitis responds well to systemic antibiotic therapy. Relieving the underlying obstruction is usually done electively but may be performed urgently in acute cases. Ophthalmic referral is necessary for this purpose.
Dacryocystitis is not uncommon in young infants who have congenital blockage of the lacrimal ducts, which often resolve spontaneously. If not, probing of the nasolacrimal system may be necessary.

Periorbital Cellulitis and Orbital Cellulitis
Periorbital (preseptal) cellulitis is a bacterial infection of the eyelids limited to the front of the orbital septum.25,26 The soft tissues around the eye are separated from the orbit by the septum, a tough membrane of protective connective tissue.
Common causes are eyelid trauma (abrasion, insect bite) contiguous infection extending from a stye or chalazion, or rarely from primary bacteremia in young infants. Common organisms are S. aureus and group A Streptococcus.
Presenting symptoms are circumferential erythema of the eyelids and periorbital skin, with swelling or puffiness of upper and or lower eyelids. Typically pain is minimal, and fever is low grade. There will be no proptosis or ophthalmoplegia. Vision is usually intact because the infection is limited to the preseptal tissues.
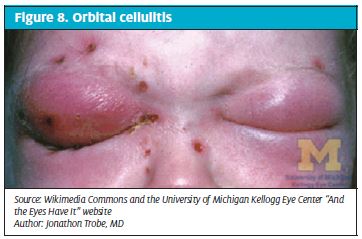
Orbital (postseptal) cellulitis (Figure 8) is a much more serious bacterial infection characterized by fever, painful purple-red eyelid swelling, and restriction of eye movement, proptosis, and variable decreased visual acuity. In general, the causative organisms are S. pneumoniae, S. aureus, H. influenzae, and Moraxella catarrhalis,. Cellulitis usually arises as a complication of ethmoid or maxillary sinusitis. Untreated orbital cellulitis can lead to blindness, cavernous sinus thrombosis, meningitis, subdural empyema, or brain abscess.
At times, it will be difficult to distinguish periorbital infection from orbital cellulitis. Computed tomography scan should generally be obtained to delineate the extent of orbital involvement. Ophthalmology consultation is advised if orbital involvement is suspected.
Except for very early periorbital cellulitis, most patients with more advanced periorbital and all those with orbital infections should be treated in the hospital with appropriate intravenous antibiotics. Underlying sinus infections also should be addressed.
References
- Mercieca K, Jones NP. Treatment of acute anterior uveitis in the community, as seen in an emergency eye centre. A lesson for the general practitioner? Eur J Gen Pract. 2012;18(1):26–9.
- Guly CM, Forrester JV. Investigation and management of uveitis. BMJ. 2010;341:c4976.
- Ishaq M, Muhammad JS, Mahmood K. Uveitis is not just an ophthalmologists’ concern. J Pak Med Assoc. 2012;62(2):92–97.
- Kruh J. Foster CS. The philosophy of treatment of uveitis: past, present and future. Dev Ophthalmol. 2012;51:1–6.
- Khairallah M, Chee SP, Rathinam SR, et al. Novel infectious agents causing uveitis. Int Ophthalmol. 2010;30(5):465–483. Goh PP, Shamala R, Chandamalar S, et al. Contact lens—related corneal ulcer: a two-year review. Med J Malaysia. 2010;65(Suppl A):120–123.
- Dethorey G, Darvich A, Hay A, et al. Severe bacterial keratitis referred to ophthalmology emergency departments: a retrospective study of 268 cases. J Fr Ophtalmol. 2012 Sep 24. [Epub ahead of print]
- Mascarenhas J, Srinivasan M, Chen M, et al. Differentiation of etiologic agents of bacterial keratitis from presentation characteristics. Int Ophthalmol. 2012;32(6):531–538.
- Srinivasan M, Mascarenhas J, Rajaraman R, et al. Corticosteroids for bacterial keratitis: The Steroids for Corneal Ulcers Trial (SCUT). Arch Ophthalmol. 2012;130(2):143–150.
- Wilhelmus KR. Antiviral treatment and other therapeutic interventions for herpes simplex virus epithelial keratitis. Cochrane Database Syst Rev. 20108;12:CD002898.
- Davis H, Mont D, Scott C, et al. Relative impact of clinical evidence and over-the-counter prescribing on topical antibiotic use for acute conjunctivitis. Br J Gen Pract. 2009;59(569):897–900.
- Yagci A, Bozkurt B, Egrilmez S, et al. Topical anesthetic abuse keratopathy: a commonly overlooked health care problem. Cornea. 2011;30(5):571–575.
- Renton BJ, Bastawrous A. Acute angle closure glaucoma (AACG): an important differential diagnosis for acute severe headache. Acute Med. 2011;10(2):77-78.
- See JL, Aquino MC, Aduan J, Chew PT. Management of angle closure glaucoma. Indian J Ophthalmol. 2011;59(Suppl):S82—S87.
- Thomas R, Walland MJ. Management algorithms for primary angle closure disease. Clin Experiment Ophthalmol. 2013;41(3):282-292.
- White J. Diagnosis and management of acute angle-closure glaucoma. Emerg Nurse. 2011;19(3):27.
- Babineau MR, Sanchez LD. Ophthalmologic procedures in the emergency department. Emerg Med Clin North Am. 2008;26(1):17-34.
- Panicharoen C, Hirunwiwatkul P. Current pattern treatment of hordeolum by ophthalmologists in Thailand. J Med Assoc Thai. 2011;94(6):721–724.
- Arbabi EM, Kelly RJ, Carrim ZI. Chalazion. BMJ. 2010;341:c4044.
- Ben Simon GJ, Rosen N, Rosner M, Spierer A. Intralesional triamcinolone acetonide injection versus incision and curettage for primary chalazia: a prospective, randomized study. Am J Ophthalmol. 2011;151(4):714–718.
- Nemet AY, Vinker S, Kaiserman I. Associated morbidity of blepharitis. Ophthalmology. 2011;118(6):1062–1068.
- Lindsley K, Matsumura S, Hatef E, Akpek EK. Interventions for chronic blepharitis. Cochrane Database Syst Rev. 2012;16(5)
- Dantas RR. Lacrimal drainage system obstruction. Semin Ophthalmol. 2010;25(3): 98–103.
- Pinar-Sueiro S, Sota M, Lerchundi TX, et al. Dacryocystitis: systematic approach to diagnosis and therapy. Curr Infect Dis Rep. 2012 Jan 29. [Epub ahead of print]
- Baring DE Hilmi OJ. Management or mismanagement of periorbital cellulitis? A review of the literature and evidenced based guide. Clin Otolaryngol. 2011;36(1):57–64.
- Pandian DG, Babu RK, Chaitra A, et al. Nine years’ review on preseptal and orbital cellulitis and emergence of community-acquired methicillin-resistant Staphylococcus aureus in a tertiary hospital in India. Indian J Ophthalmol. 2011;59(6):431–435.