
Urgent message: Though patients with posterior and bilateral epistaxis should be admitted to the hospital, the vast majority of epistaxis episodes can be treated safely and effectively in the urgent care setting.
Nathaniel Arnone, MD, Samuel M. Keim, MD, MS, and Peter Rosen, MD
Epistaxis is a common presenting complaint, with 15 per 10,000 people requiring medical attention each year.1 While the presence of blood in the pharynx can cause concern for both patients and the medical personnel treating them, the vast majority of epistaxis episodes can be successfully managed during the presenting episode, and will not require admission or specialty consultation.
Anterior vs. Posterior Origin
It is useful to classify epistaxis as either anterior or posterior in origin.
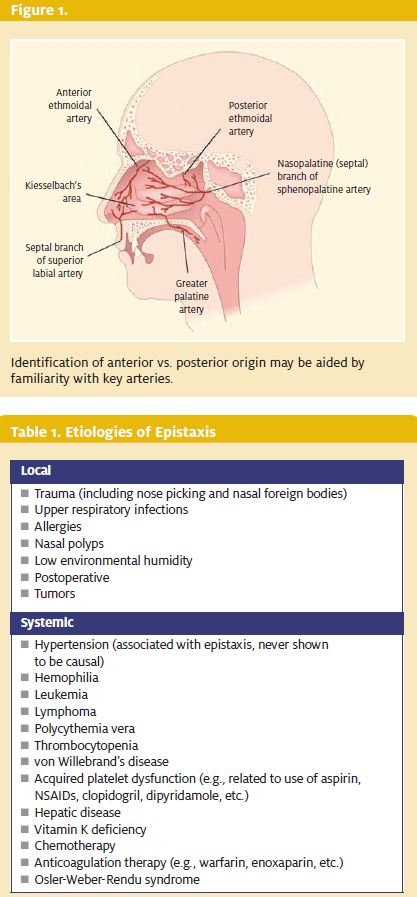
Ninety percent of all epistaxis episodes are anterior, and can usually be managed successfully with a combination of direct pressure, topical vasoconstrictors, cautery, and packing.2 Most commonly, anterior epistaxis involves Kiesselbach’s plexus, the area of vascular anastomoses of branches from the superior labial artery, the greater palatine artery, the anterior ethmoid artery, and the sphenopalatine artery (Figure 1.)
Posterior epistaxis usuallyarises from the sphenopalatine artery. Even if the bleeding appears controlled with a posterior pack, these patients require hospital admission. They have a high rate of recurrent bleeding, as well as the potential for the major complications of the posterior pack, e.g., apnea, purulent sinusitis, and superior sagittal venous plexus thrombosis.
Children rarely have a posterior bleed. Their epistaxis is almost always from a too-dry mucus membrane. Management is almost always simple and easily obtained with direct pressure. Both nares should be filled with petroleum jelly, and the parents instructed to reapply morning and evening for several days. Excessive use of this may cause risk for lipoid pneumonia.
Traumatic epistaxis from a direct blow is common but usually self limited, even when the nose is fractured.
If the septum is deviated, the patient should be seen by an otorhinolaryngologist soon because it is often easier to replace the septum acutely. The nasal mucosa must be examined to be sure there is no septal hematoma that needs to be drained, because this can increase pressure which can lead to septal necrosis.
A laceration over the bridge of the nose must be assumed to indicate an open fracture, and the patient treated with antibiotics.
History
Patients should be asked about the onset, timing, and frequency of the bleeding. They should also be queried about any trauma or other contributing factors, such as hyper- tension, rhinitis, nasal polyps, nasal foreign bodies, anticoagulation and antiplatelet ther- apies, liver disease, thrombocytopenia, or a history of bleeding diatheses (Table 1).
While there is an association between hypertension and epistaxis, no cause- and-effect relationship has been proven, to date. In one study, there was no difference in the frequency of hypertension in patients with and without epistaxis.3
The fact that the blood pressure is elevated when the patient is having an episode of epistaxis does not necessarily mean that the patient has hypertension.
The treatment of a nosebleed in a hypertensive patient is the same as in a normotensive patient. Often, the elevated blood pres- sure will return to normal with control of the bleeding. Moreover, there are no data indicating that patients who do have hypertension have higher incidence of epistaxis than do patients with no history of hypertension.
The patient will usually be able to describe which naris is bleeding. However, often patients do not know whether direct pressure will control the bleeding because many home remedies are used for epistaxis, a favorite one being to apply ice to the nape of the neck.
Physical Examination
Appropriate management of epistaxis is dependent upon localizing the source of bleeding, which requires a good light source and good exposure.
Patients should be placed in a chair that has the ability to recline, but should sit upright if possible to minimize swallowed blood. A bright external direct light source and a nasal retractor should be used to visualize the anterior nasopharynx. Most physicians will not be adept or comfortable with a reflecting mirror, and fore- head lamps are readily available (Figure 2). Clots may be removed manually or with good suction.
Once the naris is cleared, it is worthwhile to take the time to anesthetize the nasal mucosa topically. In the past, cocaine was used, but this is rarely readily available today. A solution of 4% lidocaine can be used, and is more effective when combined with a vasoconstricting agent such as neosynephrine or ephedrine.
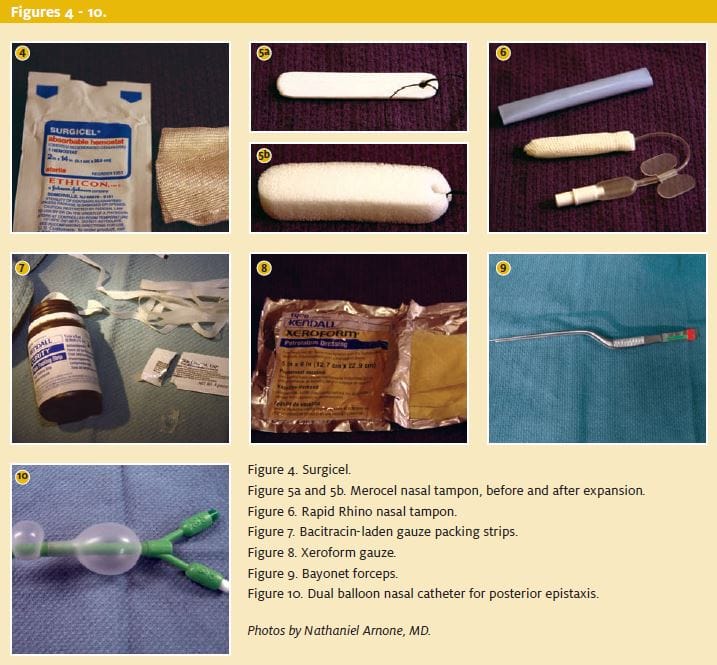
To achieve the best visibility, soak small cotton balls in a topical vasoconstrictor such as oxymetazalone, phenylephrine, lidocaine-epinephrine, or 4% cocaine (if available), and place them in the affected naris for 10 to 20 minutes. The Frazier suction catheter (Figure 3) should be used to clear the view of remaining or fresh blood while the patient is being examined. A nasal speculum is placed in the affected naris, and the anterior nasopharynx is inspected for sources of bleeding. If a nasal speculum cannot be obtained, transfer the patient to the ED, where they will have appropriate equipment. There is simply no point in trying to manage epistaxis without appropriate equipment and lighting. If the bleeding is very diffuse or rapid, congenital or acquired coagulopathies should be considered, and appropriate laboratory studies can then be performed.
Direct pressure should be held manually by medical personnel using fingers, a commercially available nasal clamp, or by taping two tongue depressors together to create a make-shift nasal clamp (sometimes referred to as the Parkland clamp). It is not helpful to ask the pa- tient to hold the pressure, since the discomfort they experience is likely to discourage them from applying enough force to stop the bleeding. Since bleeding lasts two to five minutes even in normal patients, don’t expect bleeding control in less than five minutes. Direct pressure is also not effective so long as there are clots in the naris.
Treatment
While a simple anterior bleed is easy to control, not every anterior bleed will be simple, and some will require transfer to the emergency department. Likelihood of transfer is determined by:
- bilateral bleeds
- age of the patient (<2 years or >60 years)
- history of prior recent episodes
- presence of tumor
- presence of vigorous bleeds
- early recurrence of bleeding
- suggestion of posterior or combined anterior and posterior bleeding
- underlying
Infrequently, some cases of severe epistaxis will require endotra- cheal intubation and surgical control.
Blood transfusion is rarely necessary for anterior bleeds, but may be needed to control a posterior bleed.
Reversal of anticoagulation is rarely necessary, although its presence does complicate management. Any patient who is anticoagulated those taking heparin, enoxaparin, warfarin, and the platelet inhibitors—should be transferred to the ED for management. One study finds that only three of 1,065 patients seen at an anticoagula- tion clinic over a two-year period have epistaxis requiring reversal for supratherapeutic anticoagulation.4
Patients should not blow their nose, nor pick out the clots (though they may be tempted due to significant irritation). Clots should be re- moved by suction, or manually with a nasal forceps.
Chemical Cauterization
If an anterior source of bleeding has been identified, chemical cau- terization can be attained by using silver nitrate sticks.
First, the area should be anesthetized with a topical application of 4% lidocaine. The bleeding source should be suctioned and the area made as dry and free of blood as possible.
The end of the silver nitrate stick is placed in contact with the nasal mucosa and rolled over the target for approximately five to 10 seconds. The nitric acid formed by the reaction of silver nitrate with water causes cauterization. The mucosa under the silver nitrate will immediately turn silver-gray.
Placement for longer periods of time and cauterizing both sides of the nasal septum carry an increased risk of nasal septal perforation.5 After cauterization, a topical antibiotic ointment should be generously applied to the area. Petroleum jelly can be substituted. This keeps the mucosa moist, and prevents scabbing and harsh blood clots that may irritate patients and give them the urge to pick the clots out.
Electrocautery can be attempted if the silver nitrate doesn’t work, but requires some special technique. The metal suction tip cannot be used since it will transmit the electric current, and lead to necrosis of the nasal septum. Suction can be achieved by using a glass dropper, since glass does not transmit the electric current. The coagulation current should be used on the cautery, and should be held for only a few seconds.
Absorbent Gelatin Foams, Oxidized Cellulose, and Nasal Tampons If there is bleeding from multiple small anterior sites, or if bleeding recurs after cauterization, an absorbent gelatin foam product such as Gelfoam (Pfizer) or oxidized cellulose such as Surgicel (Johnson & Johnson; Figure 4) may be used.
If cautery or absorbent sponges are ineffective, the anterior septum should be packed to provide hemostasis. Packing is uncomfortable for the patient, and analgesia and anxiolytics will be necessary. Remove any clots that have formed, and reapply a topical anesthetic and vasoconstriting agent.
Several commercial nasal tampon products are available, and may be easier to use than traditional nasal petroleum jelly-impregnated gauze packing strips. If these are used, they must be layered into the entire naris, starting at the base of the naris and continuing until the superior naris is full. The initial and the tail ends of the packing should be left outside of the naris, where they can be taped to the face to prevent the patient from in- haling and suffocating on the packing while sleeping. Merocel (Medtronic Solon) is an absorbent nasal tampon made of polyvinyl acetate that will expand when wet to become much larger than its packaged diameter (Figures 5a and 5b). The tampon is first lubricated with surgical lubricant or viscous lidocaine, and gentle pressure is applied in an anterior-to-posterior direction along the floor of the nasopharynx. The tampon should be inserted fully; however, it should not be forced if resistance is met.
Rapid Rhino (ArthroCare) is an absorbent nasal tampon that surrounds a small inflatable cuff (Figure 6). It is inserted in a fashion similar to Merocel tampon, and the cuff is inflated with air. Care should be taken not to over-inflate the cuff, so as to avoid pressure necrosis. If no commercial products are available, the nasopharynx may be packed with bacitracin laden gauze packing strips (Figure 7), or with Xeroform (Kendall Healthcare; Figure 8).
Using bayonet forceps (Figure 9), the first layer of packing is laid on the nasopharyngeal floor and advanced to the posterior wall. The next layer is then laid on top, returning in an anterior direction. The layers are stacked in an accordion fashion until the nasopharynx is completely filled. One study finds that Nu Gauze (Johnson & Johnson) packing that is pretreated with topical bacitracin grows significantly more Staphylococcus aureus than the Merocel tampon.6
It is a common but unproven practice to prescribe prophylactic oral antibiotics to patients who have been packed to prevent obstructive sinusitis or the toxic shock syndrome. Common choices would include amoxicillin or cephalexin. Packing is typically left in place for 48 hours. If bleeding continues despite adequate packing placement, the contralateral side should be packed, as well.
These patients should be admitted to the hospital. Not only is there a great risk of further rebleeding, but bilateral packing can induce apnea in some patients, and has a much higher risk of being complicated by bacte- rial sinusitis.
Posterior epistaxis often presents with bleeding that drains down the back of the patient’s throat, with a source of bleeding posterior to the middle turbinate or in the superior posterior nasopharynx.7 If anterior pack- ing is successfully placed for a suspected anterior bleed, and the patient continues to have significant bleeding, posterior packing should be placed.
Rapid Rhino also markets an anterior/posterior inflatable commercial tampon. This product is longer than the anterior tampon, but is placed in the same manner. Additionally, a dual balloon nasal catheter can be used (Figure 10). First, the nasopharynx is anesthetized and surgical lubricant or viscous lidocaine applied to the dual balloon. The catheter is inserted into the affected naris with gentle pressure until the distal balloon is visible in the patient’s mouth. The distal balloon is then inflated with 5 mL to 10 mL of sterile saline, and the proximal catheter is gently pulled back through the nose until the balloon seats itself into the posterior nasopharynx.
Next, the larger proximal cuff is inflated with 15 mL to 30 mL of sterile saline to prevent caudal migration of the catheter. Care should be taken to avoid overinflation of the catheters to prevent pressure necrosis. Additionally, the catheter should be padded with gauze where it exits the naris.
If a commercial device is not available, a Foley catheter can be used in a similar manner. The Foley is inserted into the nasopharynx and advanced until the distal end is visible in the patient’s mouth. The balloon is inflated with 15 mL to 30 mL of saline and the catheter is pulled back through the nose until the balloon is seated in the posterior nasopharynx. An umbilical clamp can be placed on the proximal end of the Foley to prevent it from slipping caudally. The umbilical clip should be padded with gauze to prevent skin breakdown.
Posterior Packing
Patients with posterior packing should be admitted to the hospital for observation and definitive treatment by an otolaryngologist. Typically, packing is left in place for 48 to 72 hours.5 Complications from posterior packing can include airway obstruction, pressure necrosis, aspiration, infection, toxic shock syndrome, and the controversial “nasopulmonary reflex,” which was thought by some to account for a decrease of PO2 and an increase in PCO2.
At least two studies find no clinical evidence of a nasopulmonary reflex in patients with posterior pack- ing.8,9 Nevertheless, there have been cases of patients found dead with posterior packing in place, with the death thought to be secondary to apnea.
Summary
Epistaxis is a common presenting complaint that can of ten be managed successfully upon the first presentation. Bleeding is usually from anterior sources and is usually amenable to direct pressure, cauterization, or nasal packing.
References and Suggested Reading
- Josephson GD, Godley FA, Stiema Practical management of epistaxis. Med Clin North Am. 1991;75:1311-1320.
- Wurman LH, Sack JG, Flannery JV Jr, et The management of epistaxis. Am J Oto- laryngol. 1992;13:193-209.
- Weiss Relation of high blood pressure to headache, epistaxis, and selected other symptoms. N Engl J Med. 1972;287:631-633.
- Nitu IC, Perry DJ, Lee Clinical experience with the use of clotting factor con- centrates in oral anticoagulation reversal. Clin Lab Haematol. 1998; 20:363-367.
- Tan LK, Calhoun Epistaxis. Med Clin North Am. 1999;83:43-56.
- Breda SD, Jacobs JB, Lebowitz AS, et Toxic shock syndrome in nasal surgery: A physiochemical and microbiologic evaluation of Merocel and NuGauze nasal pack- ing. Laryngoscope. 1987;97:1388-1391.
- Koh E, Frazzini VI, Kagetsu Epistaxis: Vascular anatomy, origins, and endovas- cular treatment. AJR Am J Roentgenol. 2000;174:845-851.
- Jacobs JR, Levine LA, Davis H, et Posterior packs and the nasopulmonary reflex. Laryngoscope. 1981;91:279-284.
- Loftus BC, Blitzer A, Cozine Epistaxis, medical history and the nasopulmonary reflex: What is clinically relevant? Otolarnygol Head Neck Surg .1994;110:363-369.

Peter Rosen, MD
