
Urgent message: Acute injuries to the foot often send patients to an urgent care center—though on occasion they don’t present for weeks, or even months, after the injury occurred. Understanding the natural history of untreated fractures in the foot is imperative to positive outcomes. The first in a two-part series.
Phillip H. Disraeli MD, FAAFP
This article will focus primarily on two aspects of care:
1. Proper management of and follow-up for simple nondisplaced fractures in the foot.
2. The role of the urgent care clinician in patients with other significant fractures, the vast majority of whom will need to be referred to orthopedics for definitive care; this will include pitfalls to avoid in the acute assessment and management of these patients.
The scope of foot fractures seen in the urgent care setting varies by locale and demographics of the patient population. For example, young families in suburban areas are more likely to present with forefoot fractures and stress fractures; in more urban or industrial environs, urgent care clinicians are more likely to see injuries resulting from motor vehicle accidents or high-energy trauma leading to fractures and dislocations of the more rigid midfoot and hindfoot.
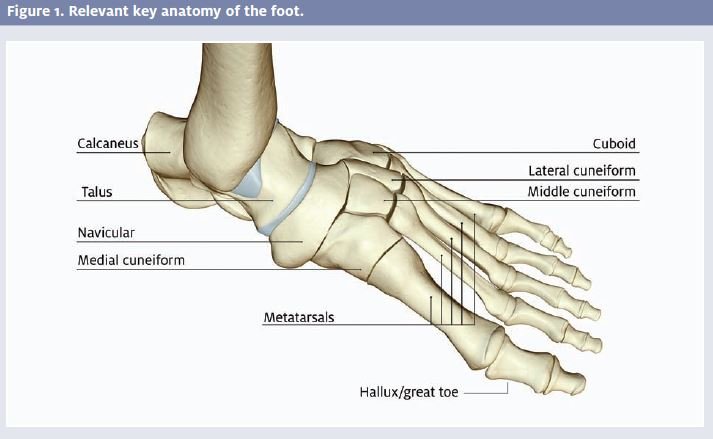
Our examination of foot fractures in urgent care will be divided into two parts. In this first installment, we will discuss fractures of the toes, meta tarsals, and Lisfranc joint (tarsal-metatarsal joints); the second will appear in the January issue of JUCM and focus on injuries, particularly fractures, to the cuboid, cuneiforms, navicular, talus, Chopart joint, and calcaneus, as well as compartment syndrome.
Great Toe (Hallux)
The great toe, or hallux, and its metatarsal are anatom ically distinct from the rest of the forefoot and are designated as the first ray. The first ray is essential to proper ambulation, especially during toe push off.
Fractures of the hallux commonly occur from a direct blow to the foot. The strong flexor tendons on the plantar surface of the toe may cause the fracture to displace and lead to chronic deformities and shoe-fitting problems if not fixed properly.
A simple, nondisplaced fracture of the distal phalanx can be treated with buddy taping of the toes for two to three weeks and a post-op shoe. However, transverse frac- tures through the proximal phalanx are more trouble- some. These should be immobilized with a CAM walker—a high-top walking boot—for two to three weeks before converting to a rigid shoe.
Because of their anatomic importance, displaced frac- tures of the proximal phalanx need to be fixed with a K wire and should be referred to orthopedics or podiatry. Due to the crush mechanism of injury, the clinician should check carefully for nailbed lacerations and a subungual hematoma.
Fractures that extend into the first metatarsophalangeal (MTP) joint space will often lead to chronic stiffness of the MTP joint. Luckily, most patients can compensate and adapt to some stiffness in this joint if the remainder of the foot has normal mobility. Displaced fracture fragment requires open fixation. Otherwise, minimal involvement of the first MTP joint can be managed with a CAM walker for three weeks, followed by a rigid post-op shoe.
The lesser toes are not as important, anatomically. The majority of fractures to these toes are the result of a direct blow or stubbing the toes while barefoot. The urgent care clinician can usually manage these injuries on site. Lacerations should be examined, cleaned, and repaired first.
A fracture dislocation or displaced fracture, if revealed by x-ray, can usually be manipulated without anesthesia and the toes buddy-taped. The patient should be advised to keep them taped for three weeks, and to wear a rigid shoe. It is expected that patients can convert to a comfortable shoe after three weeks, with eventual healing in six weeks in most cases.
Amputations of the lesser toes should be immediately referred to the ED for management.
Sesamoids of the Great Toe
The sesamoid bones of the great toe lie within the substance of the flexor hallucis brevis tendon sheath and bear up to 50% of the body weight, experiencing even greater forces during jumping activities. Their purpose is to reinforce the tendon during push-off of the toe. They also assist by elevating the first metatarsal off the ground. These sesamoids are bipartite in 25% of patients. Acute fractures may occur when landing on the ball of the foot. Stress fractures are usually the result of repetitive activities that involve landing on the toes, such as ballet, basketball, and volleyball.
CT scan or bone scintigraphy may be necessary to identify the fracture.
Differential diagnosis of sesamoid pain includes sesamoiditis, bursitis, and nerve entrapment in the area. Typically, the fracture responds well to modified activities, elimination of jumping, and a post-operative shoe for four to six weeks.
Freiberg’s Infarction
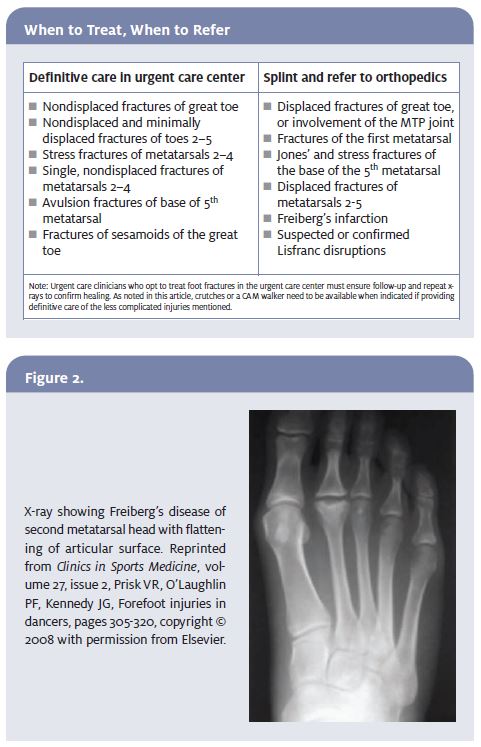
An important entity for the urgent care practitioner to be aware of when considering forefoot pain is Freiberg’s infarction (Figure 2). This is a type of osteonecrosis that occurs in the meta- tarsal heads, especially the second, and is more frequent in women.
As the infarction progresses, the metatarsal head collapses down, causing progressive metatarsalgia. The patient presents with pain and swelling in the ball of the foot. Typically, x-rays are negative at first, as the radiography often lags behind the infarction by up to six months. A high index of suspicion should prompt
the clinician to consider an MRI or bone scan. When diagnosed early, the infarction can be managed conservatively with modification of activities and a post-op shoe. If the infarction has progressed to collapse of the metatarsal head, however, the patient should be referred for arthroplasty.
Metatarsal Fractures
Weight is borne in six contact points of the forefoot the two sesamoids of the great toe and the four lesser metatarsal heads. When assessing injuries of the metatarsal region of the forefoot, the urgent care practitioner should consider three separate zones for mechanisms of injury and treatment:
The first is the first metatarsal, part of the first ray already mentioned. The second combines the second through the fourth metatarsals. These are relatively rigid, with several muscular attachments. The third is the fifth metatarsal, which is all-important because of the unique attachment of the peroneus brevis tendon laterally and the propensity for non-union in some fractures.
Typically in metatarsal fractures, patients cannot tolerate any displacement in the dorsal or volar plane due to weight bearing. Therefore, any fracture that might lead to this angulation in the sagittal plane should be referred to orthopedics.
Systematic exam
A systematic exam of the area is crucial. First, axially load each toe. Then palpate each bone, and try to sublux each joint, if tolerated. Check the neurovascular status of the foot and capillary refill to ensure good perfusion.
Remember that injuries to the area lead to swelling on the dorsal aspect of the foot because the tissue is looser on that side. However, bruising will vary, so check the sole of the foot. Standard three-view x-rays of the foot (anteroposterior [AP], lateral, and oblique) are usually ad- equate to show fractures of the area. The lateral view is especially important to rule out sagittal displacement. Although most metatarsal fractures are effectively treated conservatively, surgery is typically considered in the face of severe displacement, multiple fractures, intra-articular injury, open fractures, compartment syndrome, abnormal skin tension, significant sagittal displacement in any ray, or significant transverse displacement in the border rays.
First metatarsals
For first metatarsal fractures, one must remember that a third of the body weight is borne through this area; this is a disproportionate amount, considering the size of the first ray. Even nondisplaced fractures have to be treated with non-weight bearing for up to four weeks. Most of these will be casted, with a few treated in a CAM walker if reliably stable. Therefore, all first metatarsal fractures need to be referred to orthopedics. The displaced and intra-articular fractures will require screw fixation.
The patient will be able to tolerate some medial or lateral displacement, but no displacement in the AP direction should be considered acceptable. The urgent care clinician should place the patient in a posterior splint, order non-weight bearing, and refer to orthopedics.
Second through fourth metatarsals
For acute fractures of the second through fourth metatarsals, conservative treatment is permissible if the fracture is single and nondisplaced with no other injuries. (Remember that the metatarsal heads must be even during weight-bearing.) Treatment options for the urgent care clinician include a CAM walker or post- operative shoe, for a total of six weeks of protected weight-bearing. Careful follow-up is necessary to ensure healing, with x-rays every two weeks.
Keep in mind that dorsal or volar angulation can occur during healing due to the strong pull of surrounding muscles and ligaments. If not treated, this angulation leads to metatarsalgia or painful calluses. Medial and lateral angulation of the lesser metatarsals can also cause interdigital nerve impingement.
Fractures with more than 3 mm of displacement will require operative re- pair. Multiple fractures should be re- ferred to orthopedics.
The key to stress fractures of the second to fourth metatarsals is proper recognition. Stress fractures have a different mechanism of injury. Whereas acute fractures are a result of a direct blow or twisting trauma to the foot, stress fractures are the result of repeated microtrauma, sometimes with underlying ab- normal anatomy.
Stress fractures of the metatarsal are also known as “march” fractures because they are relatively common among military recruits. However, any person experiencing an abrupt increase in the intensity and frequency of walking or running may develop a stress fracture. Special populations include athletes, runners, and dancers. Eighty percent of stress fractures in the foot occur in the second or third metatarsal.
Another common cause of stress fracture of the fore- foot is a tight gastrocnemius muscle, which forces too much weight onto the forefoot. Other patients may be putting too much stress over a certain part of the foot (in- stead of equally distributing it) as a result of obesity, leg misalignment, or a sudden change in activity level, shoe wear, or walking surface.
Palpation of the forefoot may reveal body tenderness of the shaft of the metatarsals. Testing vibration of the surrounding bone with a low tuning fork can elicit pain at the fracture site and raise the index of suspicion.
Once diagnosed, stress fractures usually respond to modification of activities for four weeks, with special care to avoid running and jumping. Patients should wear a post-operative shoe during healing.
Fifth metatarsal
The fifth metatarsal is unique in comparison with the other metatarsals for a number of reasons:
- It is the only one with extrinsic tendon attachments; the peroneus brevis and tertius attach at its base.
- It has strong ligamentous attachments from the plantar
- It is the most mobile of the
- Most importantly, there is a tenuous vascular sup- ply to the base that impacts bone healing in the
All these factors come together to make the base of the fifth metatarsal the most difficult to assess and critical to treat for urgent care clinicians.
X-rays of the fifth metatarsal must be viewed carefully, with a hot light and magnifier being most helpful.
In children, one should note the existence of an apophysis on the base of the fifth metatarsal; it runs parallel to the base, and can be easily confused with an avulsion fracture. However, avulsion fractures run perpendicular to the shaft. The apophysis is first seen in girls aged 9 to 11 years and boys aged 11 to 14 years. This apophysis usually disappears two to three years after appearance, with bone maturation.
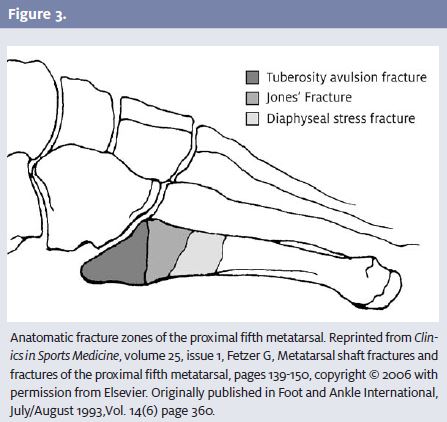
The clinician should focus on the typical locations for fractures of the base (Figure 3).
- First, there is an avulsion type of Controversy exists as to the exact mechanism of injury for these avulsions; i.e., is it the peroneus brevis tendon or the plantar aponeurosis causing the avulsion?
These avulsions are seldom displaced and are caused by inversion of the foot or ankle. Avulsion fractures are usually treated non-operatively with a CAM walker or surgical shoe, depend-ng on patient tolerance. Radiographic healing is prolonged, so the patient should be treated clinically. Most people will require some immobilization for six to eight weeks, until the fracture site is non- tender.
- A second type is the Jones’ fracture, which occurs at the junction of the diaphysis and metaphysis in the proximal fifth
This region is notorious for poor healing because of a poor blood supply, leading to more non-unions. However, the healing rate is actually higher than re- ported because previous studies had pooled data with stress fractures of the metatarsal.
Nondisplaced or minimally displaced fractures can be treated for six weeks in a non-weight bearing short leg cast, after which weight bearing is gradually increased over the next two weeks. Most frac- tures treated with this regimen go on to successful union.
Displaced fractures require screw fixation by orthopedics. The third type of fracture of the fifth base is a stress fracture; most of these patients will have some prodromal symptoms of pain in the
- The most common error found among urgent care and emergency clinicians is not recognizing the Jones’ fracture and then failing to place the patient on crutches.
The fracture probably occurs in the metadiaphy- seal region because it is the transition zone for both vascular supply and tendon forces. The bone here remains relatively avascular in comparison with its proximal and distal ends (a watershed area), and its area is an interface between the proximal attachment and pull of the peroneus brevis and the distal influence of the adductor muscles.
Therefore, most stress fractures of the proximal fifth metatarsal should be treated like a Jones’ fracture, with a non-weight bearing cast and crutches. This is distinct from stress fractures of the other metatarsals. If the x-ray shows any sign of sclerosis at the fracture margins, it will likely not heal with simple immobilization, but require screw fixation and bone grafting.
Acute fractures of the shaft of the fifth heal well with a CAM walker or surgical shoe. Patients can tolerate a little more displacement in this area be- cause of the mobility of the bone.
Lisfranc Injuries
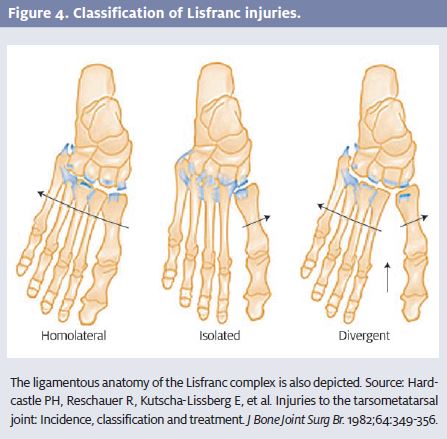
The joint between the rigid tarsal bones and the more mobile metatarsal bones is called the tarsal-metatarsal, or Lisfranc, joint; the Lisfranc disruption is an important injury pattern in the midfoot. This joint contains articulations between the cuboid and fourth and fifth metatarsals on the lateral side, and between the cuneiforms and their respective first to third metatarsals on the medial side.
The Lisfranc ligament may be injured by direct crush- ing blow or high-energy impact. A typical mechanism is for the patient to sustain a heavy axial load onto the heel while the forefoot is planted on the ground in dorsiflex- ion, i.e., a football player has his forefoot planted in the turf and another player lands across the heel. This injury may also occur in motor vehicle accidents.
In general, single Lisfranc joint disruptions are more common with sports injuries and multiple disruptions occur with motor vehicle accidents. Typically, the patient will present with pain in the midfoot, pain with weight bearing and inability to walk on their toes. Inspection of the foot will reveal dorsal swelling and ecchymosis of the midfoot. During palpa- tion, the clinician will note tenderness of one of the tarsal-metatarsal articulations.
If the patient can tolerate it, the examiner should try to stress the individual tarsal-metatarsal joints. This is performed by holding the midfoot fixed and individually dorsiflexing each joint. Pain with this stress or instability compared with the contralateral side should elicit suspicion for a Lisfranc disruption.
Another useful technique is to passively pronate and supinate the forefoot. Pain with this test is highly sugges- tive of Lisfranc disruption.
In cases of suspected Lisfranc injury, careful examina- tion for a symmetric dorsalis pedis pulse is mandatory. Even more common than a dorsalis pedis interruption, however, is a disruption of the first intermetatarsal artery located in the intermetatarsal space. This injury is a common cause of compartment syndrome in the foot and should be considered in Lisfranc injuries.
Lisfranc injuries range from stretch of the ligament, to complete tear of the ligament, to associated fractures and dislocations in the region. Figure 4 shows typical Lis- franc injury patterns.
X-rays are always indicated when a diagnosis related to Lisfranc injury is being entertained. On the AP and oblique view of the foot, one should look for medial side alignment of each cuneiform with its respective metatarsal base. The fourth metatarsal should align with the cuboid bone on the medial aspect.
Reviewing the lateral film, an imaginary line drawn dorsally should align the metatarsals and their respective tarsal bones. The plain films may show a widening of the space between the first and second metatarsal bases (2 mm or more), with an associated avulsion fracture of the second metatarsal. This avulsion is referred to as the “fleck sign.”
Keep in mind that normal x-rays do not rule out a Lisfranc disruption. The joints may still be unstable and should be tested with weight-bearing films or stress radiographs under anesthesia if suspected. Some authors recommend CT scanning to better delineate the Lis- franc ligament and its supporting struc- tures. Patients with suspected Lisfranc injuries must be re- ferred to orthopedics for further evaluation. Stress radi- ographs may be necessary to determine if the Lisfranc joint is stable.
Some of these injuries are subtle but can still lead to disability. A Grade 1 sprain of the Lisfranc ligament may be treated conservatively, but any unstable ligament tear or associated dislocation must be treated operatively.
Patients will undergo open reduction and internal fixation (ORIF) and be non-weight bearing for several weeks. Even with ideal repair, 40% of patients will suf- fer some degree of disability and limp.
Urgent care clinicians should place patients with suspected Lisfranc injuries in a posterior splint with crutches and refer them to orthopedics. If there is a dislocation, neurovascular compromise, or compartment syndrome, the patient should be sent to the emergency department immediately.
Part 2, to be published in the January 2009 issue of JUCM, will resume with treatment of the midfoot and hindfoot and compartment syndrome. For Resources and Suggested Reading associated with this article, log on to www.jucm.com.
