Urgent message: Various methods have been suggested for screening for type 2 diabetes mellitus in the asymptomatic population, although more consensus about the best approach, especially in settings outside primary care, is required. The usefulness of a diabetes-screening pathway for the early detection of undiagnosed diabetes was assessed in a quality-improvement study of a convenience sample from an urgent care center. How this article/column helps you: by analyzing findings on how screening all adults for diabetes could work in your urgent care center.
Shannon R. Clark, MSN, RN, RNFA, FNP-C, and Marisa L. Wilson, DNSc, MHSc, RN-BC, CPHIMS
Abstract
Background: Undiagnosed diabetes affects over 9 million Americans, with over 79 million estimated to have blood glucose levels in the range of prediabetes. Various methods have been suggested to screen for undiagnosed diabetes in the asymptomatic population, although a consensus about the best evidence-based approach, especially in settings outside primary care, is required.
Objective: We evaluated the usefulness of a diabetes-screening pathway for the early detection of undiagnosed diabetes in in an urgent care population.
Methods: A convenience sample of 64 patients were recruited from an independent urgent care center in California for participation in a nonexperimental study. Inclusion criteria included adulthood and no prior diagnosis of prediabetes or diabetes. All participants were assessed using the Early Diabetes Detection Pathway (EDDP), a two-phase process that is based on the 2014 American Diabetes Association diabetes-screening guidelines and includes participant completion of a diabetes risk questionnaire (DRQ) and collection of diabetes diagnostic data (DDD). Participants found to be at risk were further screened using fingerstick testing of glycated hemoglobin (HbA1c) levels. To determine the pathway’s usability and feasibility in the urgent care setting, staff members were surveyed regarding their satisfaction with it.
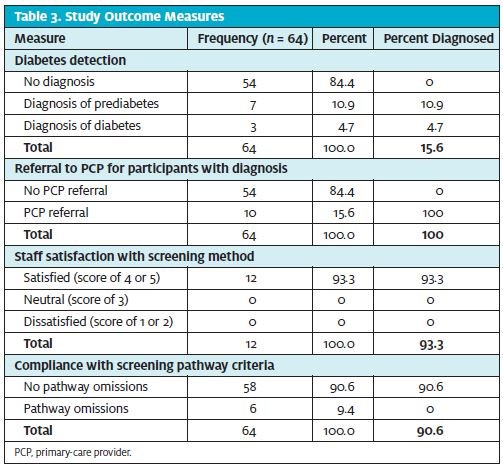
Results: At baseline, the 64 participants (100%) who met eligibility criteria had previously undiagnosed prediabetes and diabetes. An HbA1c of 5.7% to 6.4% produced a diagnosis of prediabetes in 7 participants (10.9%), and a value of 6.5% or more produced a diagnosis of diabetes in 3 participants (4.7%). Ten participants (100%) in whom prediabetes or diabetes was diagnosed were referred by the urgent care center to a primary-care provider. The survey showed that 93.3% of urgent care center staff members were satisfied with use of the pathway, with a 90.6% compliance rate with pathway criteria.
Conclusion: Use of the EDDP is an effective and feasible method for diabetes screening in urgent care centers, although study in a much larger population is necessary to confirm this finding. Early diabetes detection measures implemented in the urgent care setting will increase detection of previously undiagnosed prediabetes and diabetes and referrals to primary-care providers in patients who present to urgent care centers.
Introduction
Lack of access to established primary-care services, medical workforce shortages, and lack of time have led to a dramatic growth in the urgent care industry in order to meet the health-care demands of the nation. Urgent care centers have become one of the first-line providers for a large proportion of the U.S. population, with millions of insured and uninsured Americans presenting to urgent care centers annually for both urgent and nonurgent problems. This highlights the need for the specialty of urgent care medicine to respond by adjusting current practice standards to include both acute and chronic disease detection and management. With millions of people living with undiagnosed type 2 diabetes mellitus or prediabetes, earlier and more widespread detection and intervention are warranted to prevent the morbidity and mortality that follows.
Part 1 of this article focused on evaluation of diabetes screening for the adult urgent care patient. [See “Original Research: Early Diabetes Screening in the Urgent Care, Part 1,” at https://www.jucm.com/original-research-early-diabetes-screening-urgent-care-part-1/.] Undiagnosed diabetes affects more than 9 million Americans, with 79 million Americans estimated to have blood glucose levels in the range of prediabetes. In total, the numbers place more than 100 million Americans at risk for developing diabetes.1 In 2013 the total U.S. diabetes expenditure reached approximately $48 billion, and that is projected to escalate to over $79 billion2 by 2023. Diabetes is one of the leading causes of premature morbidity and mortality.3,4 The burden of diabetes continues to grow: The number of adults with type diabetes is projected to increase from 371 million in 2012 to approximately 552 million by 2030 worldwide.5,6 The significance in terms of health and financial impact supports the critical need to implement early diabetes detection strategies in all practice settings to reduce the long-term burden of the disease.
Effectiveness of diabetes screening in the asymptomatic patient population has been poorly described in the literature.7,8 Several studies have looked at diabetes screening in the perioperative setting.7–10 Data from this research suggests that prediabetes or diabetes would be diagnosed earlier in the disease process in millions of individuals from the screening processes described in these studies alone.7 Consistent data within the literature reveals that a high proportion of those with new diagnoses already have comorbidities, demonstrating a link between early diabetes detection and reduced future complications.7–12
In this second part of a two-part article, we discuss a study of the feasibility of early detection of prediabetes and type 2 diabetes in the fast-paced environment of urgent care. We performed the study because of the current lack of evidence regarding the diagnosis and treatment of those with impaired glycemic control in urgent care.7,8 With diabetes being a disease with severe subsequent health consequences and considering that urgent care centers provide care to much of the population, continued efforts to investigate early screening methods appropriate for the specialty of urgent care medicine are warranted.
Methods
Literature Search
We conducted an electronic literature search using PubMed, CINAHL (Cumulative Index to Nursing and Allied Health Literature), EMBASE, Cochrane Library, and Scopus. The search included articles written in English and published between 2010 and 2014. Keyword search terms elicited well over 10,000 studies across all databases. Articles that met both the inclusion and exclusion criteria were selected for analytical review, reducing the major search to approximately 200 articles. After reading the full text and performing a manual search of the reference lists, we conducted further refinements, which decreased the final count to 16 articles. The content of the 16 selected studies included diabetes statistics and recommendations for screening, diagnostic, and therapeutic actions that have been shown to favorably affect health outcomes in patients who have prediabetes and diabetes.11 The Johns Hopkins Nursing Evidence-Based Rating Scale was used to evaluate and critique the evidence. The quality and strength of the evidence was carefully assessed, allowing only good to high-level research to be used for translation into clinical management and practice discussion.
Participants and Procedures
We conducted a 3-month nonexperimental quality-improvement study using a convenience sample to determine the feasibility of diabetes screening in urgent care centers and referral from urgent care centers to primary-care providers (PCPs) for the population with disease diagnosed via the Early Diabetes Detection Pathway (EDDP) that we developed. The study was approved by the Johns Hopkins University School of Medicine Institutional Review Board. Inclusion criteria were defined as adult patients age 18 years or older presenting to Synergy Health Center and Urgent Care with no prior diagnosis of prediabetes or diabetes. All participants meeting inclusion criteria were invited to enroll in the study and were provided information about it and then indicated their consent in writing.
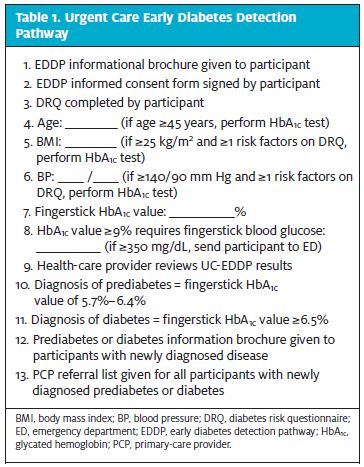
All participants underwent assessment with the EDDP (Table 1), a two-phase pathway that included participant completion of a diabetes risk questionnaire ([DRQ] Table 2) and collection of diabetes diagnostic data (DDD). The 2014 American Diabetes Association diabetes-screening guidelines were used as a foundation to design the pathway criteria.11 Study participants determined to have a positive diabetes risk on the basis of results from the DRQ and DDD were further screened by fingerstick testing for glycated hemoglobin (HbA1c) levels to detect prediabetes or type 2 diabetes. The final stage of the study included a staff satisfaction survey and evaluation of pathway compliance to determine feasibility in the urgent care setting.
 Measurements
Measurements
Data were collect by local health-care providers from August 1, 2015, until October 31, 2015, at one of the Synergy Health Center and Urgent Care sites, which are independent urgent care centers in Northern California. All adults who presented for care at the urgent care center and in whom diabetes had never been diagnosed were invited to participate in the study. Clinic staff members recorded patient consent, administered the DRQ, and collected DDD. The DDD included documentation of participant age, body mass index (BMI), and blood pressure (BP). Testing was conducted to detect diabetes and prediabetes in asymptomatic adults who (1) were overweight or obese, with a BMI ≥25 kg/m2, combined with one or more risk factors on the DRQ, and/or (2) had elevated BP with a reading of ≥140/90 mm Hg, with one or more risk factors on the DRQ. For those age 45 years and older, testing was conducted regardless of BMI, BP, or DRQ results.
For each participant, capillary blood HbA1c concentration was measured in a fingerstick blood sample collected by health-care providers and analyzed on a calibrated Siemens DCA/2000 Analyzer. The Siemens point-of-care machine is a standard in the industry and is routinely used for detecting diabetes. The aim of the study was to evaluate effectiveness and feasibility of using the pathway in a real-world urgent care setting, so we believed that rapid HbA1c testing was the most appropriate and reliable test. HbA1c measurement does not require fasting, and values provide an established measure of long-term glycemic control that is not affected by transient hyperglycemia from acute stress or illness.13
American Diabetes Association diagnostic criteria were used to evaluate participants’ HbA1c values to diagnose prediabetes or diabetes. An HbA1c range of 5.7% to 6.4% produced a diagnosis of prediabetes, and a cutoff of ≥6.5% produced a diagnosis of diabetes.11 Participants identified as having HbA1c values ≥9% underwent measurement of capillary blood glucose levels in a fingerstick blood sample by a calibrated glucometer. Participants whose blood glucose levels measured ≥350 mg/dL were sent to a local emergency department (ED).
Results of the DDD were reviewed by health-care providers with all participants. Participants in whom prediabetes or diabetes was diagnosed were given handouts on diabetes and a list of PCPs so that they could arrange for follow-up care. At the conclusion of the study collection period, a staff satisfaction survey using a six-question Likert rating scale was administered to all study team members to evaluate satisfaction with utilization of the pathway in the urgent care center.
 Results
Results
A total of 64 adult patients presenting for care at Synergy Health Center and Urgent Care in Pleasanton, California, in whom diabetes had never been diagnosed were recruited for participation in the urgent care EDDP (UC-EDDP). Participant ethnicity was as follows: 71.9% White/non-Hispanic, 12.5% Asian, 12.5% Hispanic, 3.1% African American. Of the participants, 43.8% were men and 56.3% were women, and their age ranged from 23 to 71 years (mean, 45 years). Participant payor mix was as follows: 61% privately insured, 19% cash, 12% workers’ compensation, and 8% Medicare.
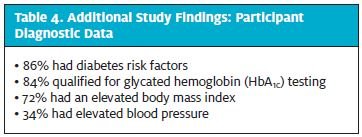
At baseline (Table 3), 64 participants (100%) had previously undiagnosed prediabetes or diabetes. An HbA1c range of 5.7% to 6.4% produced a diagnosis of prediabetes in 7 participants (10.9%). An HbA1c of ≥6.5% produced a diagnosis of diabetes in 3 participants (4.7%). Ten participants (100%) with diagnosed prediabetes or diabetes were referred from the urgent care center to a PCP. Of the 12 (n = 12) urgent care center staff members surveyed, 93.3% were satisfied with use of the pathway, and there was a 90.6% staff compliance rate with pathway criteria. Additional study findings (Table 4) identified 55 participants (86%) with positive findings for diabetes risk factors, 54 participants (84.4%) qualifying for HbA1c testing, 46 participants (71.9%) with an elevated BMI, and 22 participants (34.4%) with elevated BP.
Discussion
The data demonstrate that 15.6% of the 64 participants screened had previously undiagnosed, asymptomatic prediabetes or diabetes. Given the opportunity to expand this screening method to a larger scale, we could be identifying millions with diabetes substantially earlier in the disease process. Earlier diagnosis and treatment would lead to reduced complications, improved health, and a dramatic reduction in diabetes financial expenditures. Improved screening measures using the EDDP will also serve to reduce unnecessary visits to an ED for undiagnosed or uncontrolled diabetes, which alone causes significant financial burden to the system.
High staff satisfaction with the EDDP demonstrates strong feasibility in the urgent care environment. Despite the fast pace of urgent care, staff members were able to learn and adhere to the pathway criteria efficiently and effectively, as evidenced by a 90.6% compliance with the pathway. A 100% PCP referral rate for the 10 participants with diagnosed disease further establishes the importance and ability for urgent care centers to provide continuity of care between the specialties of urgent care and primary care. This also highlights the volume of patients who present to urgent care centers with chronic illness and the critical need for the population to have access to primary-care services through urgent care centers.
 Synergy Health Center provides internal primary-care services, and the majority of our study participants found to have diabetes or prediabetes elected to receive care within our facility. This provided additional opportunity to monitor and evaluate patient adherence to treatment regimens. The majority of participants with newly diagnosed prediabetes or diabetes continue to receive care at our facility and have improved health outcomes as a result of the EDDP. The data strongly demonstrate that the EDDP is an effective and feasible method for diabetes screening in the urgent care setting and will improve referral from urgent care centers to PCPs for patients with newly diagnosed diabetes or prediabetes.
Synergy Health Center provides internal primary-care services, and the majority of our study participants found to have diabetes or prediabetes elected to receive care within our facility. This provided additional opportunity to monitor and evaluate patient adherence to treatment regimens. The majority of participants with newly diagnosed prediabetes or diabetes continue to receive care at our facility and have improved health outcomes as a result of the EDDP. The data strongly demonstrate that the EDDP is an effective and feasible method for diabetes screening in the urgent care setting and will improve referral from urgent care centers to PCPs for patients with newly diagnosed diabetes or prediabetes.
The growing trend of using urgent care centers for nonurgent problems emerged as a response to increased demand for quick, accessible, and affordable care. In the past, the field of urgent care medicine was expected to provide solely episodic acute care. The urgent care center stands as one of the most evolved and established walk-in clinic models and represents two of the most recent financial cornerstones in health care: quality and value. As the standard in the convenient-care industry, urgent care must take up the next task of improving the consistency with which walk-in clinics provide treatment of chronic disease and coordinated services with primary care either internally or externally.
The Urgent Care Association of America’s 2014 Benchmarking Survey Results reveal that an average of 75% of urgent care patients have a PCP outside the center, leaving nearly 25% who may be using urgent care centers as their PCP. Approximately 26% of urgent care centers now provide formal primary care. The benchmarking survey shows that 93% of urgent care centers have a standard process in place to help patients find a regular provider, yet only 55% are actually assisted with this this task.14
Limitations
Our study was limited by a small sample size, an inherent feature of our pilot study design. As a result, we cannot generalize the results of our intervention to the large volume of patients that present to urgent care centers each year in the United States. Further implementation of our pathway in urgent care centers across the nation would allow for continued evaluation of this screening method.
 Conclusion
Conclusion
With a health-care system already faced with capacity strain, the demand for urgent care centers to provide primary-care services will continue to grow. Health-care reform has translated to an increase in the number of individuals seeking primary-care services at urgent care centers. The best way to address this problem is to implement screening modalities directed at bridging the gap between the volumes of Americans who are in need health care with those who have access only to urgent care centers for primary care. To accomplish this, urgent care providers must readjust current specialty standards to adopt new roles that include the provision of preventive care and chronic disease management.
Measures to create efficient and cost-effective ways for urgent care providers to use screening methods such as the EDDP will translate to increased disease detection and a reduction in associated complications. We demonstrated that the EDDP is an effective and feasible method for diabetes screening in the urgent care setting and will improve referral rates from urgent care centers to PCPs for patients in whom diabetes was previously undiagnosed. Data from further implementation of the pathway in urgent care centers across the United States will allow for more accurate accounting for the prevalence and incidence of prediabetes and diabetes and will provide a means for detecting diabetes earlier in the disease process.
Urgent care providers are in a unique position to provide a hybrid approach to address both acute and chronic illness by using screening methods such as the EDDP that have been studied and demonstrated to be feasible in this setting. Long-term outcomes of this practice approach will lead to dramatic improvements in the health and quality of life for those people who have diabetes and other chronic illness.
Citation: Clark SR, Wilson ML. Original research: early diabetes screening in the urgent care, part 2. J Urgent Care Med. October 2016. Available at: https://www.jucm.com/original-research-early-diabetes-screening-urgent-care-part-2/.
References
- Centers for Disease Control and Prevention (CDC). National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2011 [accessed 2013 May 8]. Available from: http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2011.pdf
- DeVol R, Bedroussian A. An unhealthy America: the economic burden of chronic disease. Santa Monica, CA: Milken Institute; © 2007 [accessed 2010 July 4]. Available from: http://assets1b.milkeninstitute.org/assets/Publication/ResearchReport/PDF/chronic_disease_report.pdf
- Pratley RE. The early treatment of type 2 diabetes. Am J Med. 2013;126(suppl 1):S2–S9.
- Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14.
- International Federation of Diabetes. IDF Diabetes Atlas. 5th ed. Brussels, Belgium: International Diabetes Federation; 2011 [accessed 2013 May 8]. Available from: http://www.diabetesatlas.org/component/attachments/?task=download&id=116
- World Health Organization. Diabetes fact sheet 312. Geneva, Switzerland: World Health Organization [published 2011 January; last updated 2016 June; accessed 2013 May 8]. Available from: http://www.who.int/mediacentre/factsheets/fs312/en/
- Sheehy AM, Benca J, Glinberg SL, et al. Preoperative “NPO” as an opportunity for diabetes screening. J Hosp Med. 2012;7:611–616.
- Wang R, Panizales MT, Hudson MS, et al. Preoperative glucose screening tool in patients without diabetes. J Surg Res. 2014;186:371–378.
- Choi SH, Park KS, Kim TH, et al. Hemoglobin A1c as a diagnostic tool for diabetes screening and new-onset diabetes prediction a 6-year community-based prospective study. Diabetes Care. 2011;34:944–949.
- Tapp RJ, O’Neil A, Shaw JE, et al; AusDiab Study Group. Is there a link between components of health-related functioning and incident impaired glucose metabolism and type 2 diabetes? The Australian Diabetes Obesity and Lifestyle (AusDiab) study. Diabetes Care. 2010;33:757–762.
- American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1): S14–S80. Available from: http://care.diabetesjournals.org/content/37/Supplement_1/S14.full
- Weinick RM, Burns RM, Mehrotra A. Many emergency department visits could be managed at urgent care centers and retail clinics. Health Affairs. 2010;29:1630–1636.
- Magee MF, Nassar C. Hemoglobin A1c testing in an emergency department. J Diabetes Sci Technol. 2011;5:1437–1443.
- Urgent Care Association of America. 2014 Urgent Care Benchmark Survey Results. Naperville, IL: Urgent Care Association of America. © 2014 [accessed 2015 December 8]. Available from: http://www.ucaoa.org/?UCBenchmarking