Urgent message: While standards for pediatric emergency care have been defined for outpatient offices and emergency departments, guidelines have not been published for urgent care centers. This study assesses the presence of equipment, supplies, and medications necessary to manage emergencies in pediatric urgent care centers.
Amanda Montalbano, MD, MPH, FAAP and Brian Lee, PhD, MPH
Results from this project were presented in poster format the Pediatric Urgent Care Conference in Orlando, FL in 2018. No funding was received for this project.
INTRODUCTION
Preparedness standards for pediatric emergencies have been established for the emergency department and outpatient offices.1,2 General emergency department preparedness for pediatric emergencies is actively monitored by the National Emergency Medicine Services for Children.3 While a national assessment of urgent care centers’ preparedness for pediatric emergencies suggested an essential equipment, supplies, and medication list based on outpatient offices,4 there is no national governing body or consensus of what equipment, supplies, and medications are necessary in an urgent care setting.
This project aimed to establish what the current inventory of equipment, supplies, and medications in specialized pediatric urgent care centers is across the United States. This information would then be used to inform policy on what essential and suggested equipment, supplies, and medications should be expected in case of pediatric emergency at these sites, with recommendations ultimately shared with the general urgent care community to provide guidance; educate referring and receiving sites of the capabilities of pediatric urgent care clinics; and guide triage to the appropriate level of pediatric care.
Methods
The Organization for Urgent Care Health (OUCH) conducts a national annual survey of specialized freestanding pediatric urgent care centers. This survey is sponsored by both the American Academic of Pediatrics Section of Urgent Care Medicine and the Society of Pediatric Urgent Care to support building a database of administrative, operational, and clinical metrics for pediatric urgent care centers. The OUCH survey distributed in December 2017 contained an addendum to collect information about the equipment, supplies, and medications on hand for emergencies at the responding site. The emergency preparedness addendum was adapted with permission from the National Emergency Medicine Services for Children data collection survey of general emergency departments.
This OUCH survey was distributed via email and postal mail to 109 pediatric urgent care centers (estimated to represent about one-third of all free-standing pediatric urgent care sites in the nation). Each invited urgent care center received a color-coded length-based pediatric measurement tape for emergencies in advance of their participation. Data were collected and managed via REDCap, hosted at Children’s Mercy Kansas City.5 Frequencies and percentages are reported and calculated using Microsoft Excel 2013. Comparison of groups were completed using Fischer’s Exact test with p-value threshold <0.05 (StataCorp. 2017, Stata Statistical Software: Release 15. College Station, TX). The project was deemed non-human subjects research by the Institutional Review Board at Children’s Mercy Kansas City.
RESULTS
Of the 109 invited pediatric urgent care sites, 67 responded to the OUCH survey (61% response rate). Of the 67 freestanding pediatric urgent care site respondents, 62 (93%) completed the Emergency Preparedness addendum. Respondents included 17 different institutions across 16 states. Almost two-thirds were hospital affiliated (62%), 37% were private organizations, and 1% were part of a managed care organization (which for purposes of the remainder of the reporting were grouped with “hospital-affiliated”).
Equipment
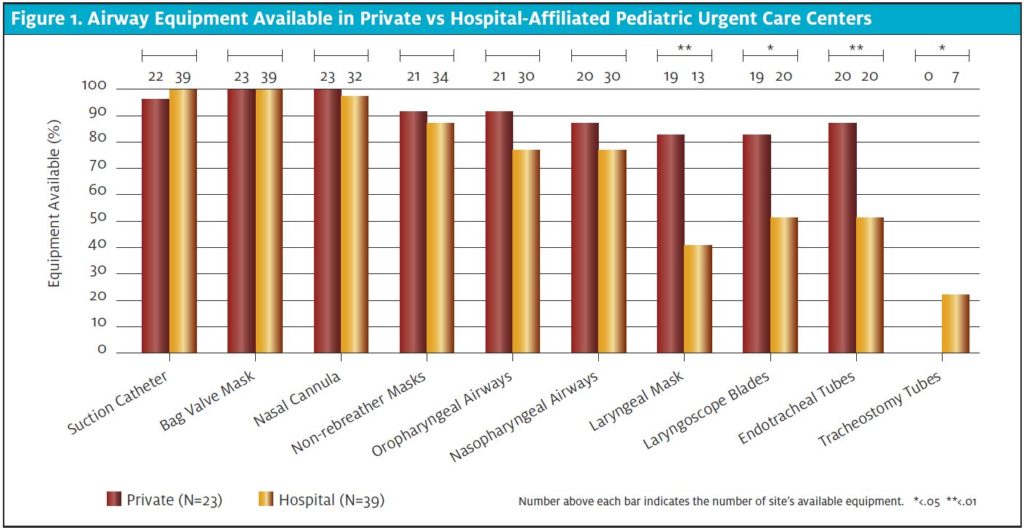
Airway equipment (ie, bag-valve mask required to deliver basic life support) was unanimously present in both hospital-affiliated and private institutions (Figure 1). Ability to perform suction (presence of any size suction catheter) and nasal cannula were almost always present (99%); however, non-rebreather mask was present less than 90% in both care settings. The ability to maintain airway patency with either an oropharyngeal (77% vs 91%; p=.187) or nasopharyngeal airway (77% vs 87%; p=.508) in hospital or private settings, respectively, did not differ significantly. However, presence of laryngeal mask airway (41% in hospital settings vs 83% in private settings; p=.002), endotracheal tube (51% vs 87% p=.006), and ability to place advanced airways (any laryngoscope blade [51% vs 83%; p=.016]) differed significantly between hospital and private settings. Ability to change out a tracheostomy was not common (0% hospital-affiliated, 22% private settings; p=.034).
Figure 1. Airway Equipment Available in Private vs Hospital-Affiliated Pediatric Urgent Care Centers
Supplies
While 100% of all respondents have supplies on hand to splint extremities or apply sterile dressings for injuries, only 95% had cervical collars available for potential spinal cord injuries. Glucometers were present in 88% of facilities. Only 84% had a small interosseous needle present to deliver resuscitative fluids or vasoactive medications in case of a code event. Just over half (54%) had a cardiorespiratory monitor. While only 34% had a defibrillator with cardioversion, 87% had an automated external defibrillator (not mutually exclusive categories). Quick reference guides like a Pediatric Advanced Life Support card (92%) and pediatric weight/length-based dosing tape (89%) were not unanimously present.
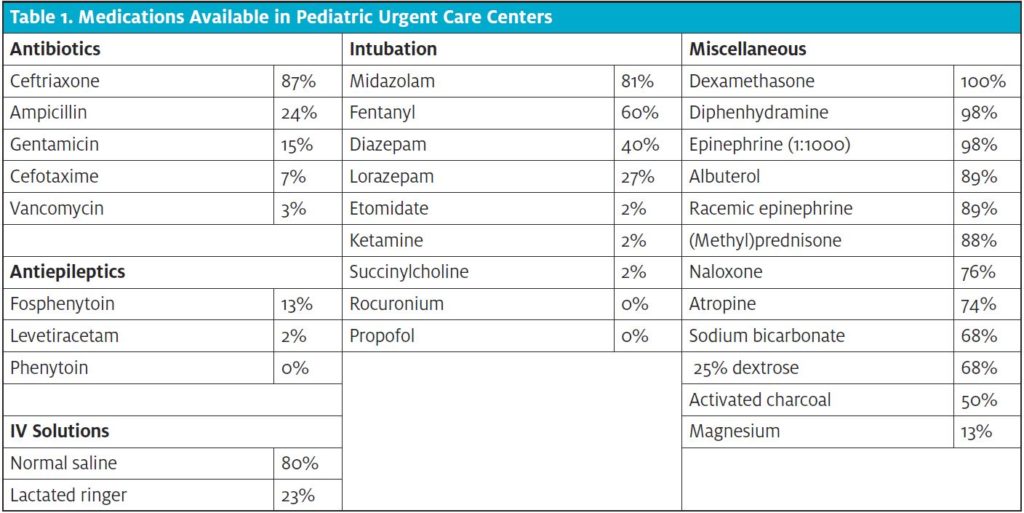
Medications The medications available in the respondent pediatric urgent care sites varied (Table 1). Ceftriaxone was the most common antibiotic available (87%). Antiepileptics (phenytoin [0%], fosphenytoin [13%], and levetiracetam [2%]) were uncommon; however, sedative medications that can also be used as an anticonvulsant (midazolam 81%; diazepam 40%, and lorazepam 27%) were sometimes present. Opioid antagonist medication, naloxone, was available in three-quarters (76%) of pediatric urgent cares. While 40 sites (60%) had airway equipment to place an advanced airway, paralytic intubation medications were rarely present (succinylcholine 2%, rocuronium 0%). Inhaled respiratory medications (albuterol and racemic epinephrine) were present in 89% of sites. The most common medications on hand were dexamethasone (100%), diphenhydramine (98%), and epinephrine (1:1000) (98%).
DISCUSSION
Pediatric emergencies can happen in any care setting, and while every office or clinic would ideally be able to diagnose, treat, and manage those emergencies there are competing priorities of cost, quality, and appropriate scope of care. However, scared families may present to the closest available site that is the most convenient, cost-effective, and efficient. The triage of patients to convenient care sites in turn place the onus on the health care facility to be prepared for a variety of not only illness and injury, but also acuity. Equipment, supplies, and medications for at least the most common pediatric illnesses and injuries should be available at all pediatric urgent care locations.
Studies have shown pediatric airway emergencies initially treated and managed in the non-intensive care setting have decreased success with first intubation attempt and led to poorer clinical outcomes.6 With private sites having increased ability to place advanced airways, it may be reasonable to assume that the providers at those sites (operating outside a hospital affiliation) have advanced training such as in pediatric emergency medicine or critical care experience.7 While advanced airway placement abilities may be variable, freestanding sites should have the capability to deliver basic life-saving protocols and every facility should have a bag-valve mask available with infant, pediatric, and adult masks. Whereas almost all sites had nasal cannulas available to deliver oxygen, this modality is more appropriate in titrating to room air or long-term oxygen delivery at low levels. In an emergency situation the use of a non-rebreather would be a more appropriate delivery model; yet, this was not as common to have on hand.
As respiratory distress, psychiatric emergencies, and seizures are the most common causes of pediatric emergencies in the outpatient setting,8 it is also concerning that certain medications were not stocked in all facilities. Beyond the respiratory support equipment like bag-vale masks, inhaled medications like albuterol and racemic epinephrine should be readily available. Another important class of medications not always present were antiepileptics. For children who present in status epilepticus, pediatric urgent care should be able to provide airway clearance, assisted respirations, diagnostic equipment such as a glucometer, and antiepileptic medications.
Beyond the most common presentations of pediatric emergencies, those that are immediately life-threatening if not identified and treated should also be taken into consideration as a high-priority. This study showed most pediatric urgent cares were prepared to treat anaphylaxis as epinephrine, steroids, and antihistamines were almost always on hand. The route of administration was not collected; therefore, it is unknown if all three medications would be able to be given in a non-oral route if the patient were not able to safely swallow.
One barrier to maintaining equipment, supplies, and medications for emergency situations is the limited shelf-life and regulations to keep the items stocked and in working order. Urgent cares frequently operate on a slim financial margin and costly equipment, supplies, and medications that will only be used in rare emergency situations may be a barrier to having them required to be on-site. Solutions to maintain in-date stock of all emergency-use medications, especially for those sites not affiliated with a hospital, need to be explored.
Adult Emergencies
While pediatric emergencies would likely be the most common emergency situations managed in a specialized pediatric urgent care center, any pediatric healthcare facility would be remiss to not be prepared to deliver basic life-saving measures to an adult.9,10 Commonly reported adult emergency presentations in the pediatric setting include various injuries, cardiac events, and syncope.10,11 Overdose is a concern in both pediatric and adult patients and just over three-quarters of pediatric urgent cares had naloxone on-hand. It would be advisable, even in a pediatric care facility, to have essential equipment, supplies, and medications on hand for adult emergencies including adult-sized respiratory masks, cervical collars, automated electronic defibrillator, epinephrine, and naloxone. Established relationships with emergency medical transport services and referring facilities for both adult and pediatric patients should also be in place.12
LIMITATIONS
This was the first national survey of emergency readiness in the pediatric urgent care setting. The data here are not representative of “fast-track” zones in an emergency room, urgent care clinics co-located with an emergency department, or after-hours clinics of a pediatric primary care office. The sample size was only 62 centers; however, there was reasonable geographic variability and institution representation of both private and hospital-affiliated sites. The data reflect significant variation in pediatric emergency equipment, supplies, and medications in specialized urgent care centers at the time of the study, which may be in part to the variation in scope of care; however, the young field of pediatric urgent care has matured and become more homogenous in scope of care in the years since.
CONCLUSION
OUCH has highlighted the need to standardize scope and standards for pediatric urgent care centers. This data collection was an important step in order to provide an understanding of the scope of care available in specialized pediatric urgent care centers. Moving forward, more efforts to establish emergency preparedness standards and staff training requirements, and to define safe pediatric urgent care, are needed.
Citation: Montalbano A, Lee B. Preparedness for emergencies in pediatric urgent care settings. J Urgent Care Med. 2020;15(1): https://www.jucm.com/preparedness-for-emergencies-in-pediatric-urgent-care-settings/.
REFERENCES
1. Committee on Pediatric Emergency Medicine. Preparation for emergencies in the offices of pediatricians and pediatric primary care providers. Pediatrics. 2007;120(1):200-212.
2. Krug SE, Bojko T, Fein JA, et al. Joint policy statement ─ guidelines for care of children in the emergency department. Pediatrics. 2009;124(4):1233-1243.
3. Gausche-Hill M, Ely M, Schmuhl P, et al. A national assessment of pediatric readiness of emergency departments. JAMA Pediatr. 2015;169(6):527.
4. Wilkinson R, Olympia RP, Dunnick J, Brady J. Pediatric Care provided at urgent care centers in the united states: compliance with recommendations for emergency preparedness. Pediatr Emerg Care. 2016;32(2):77-81.
5. Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap) – A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inf. 2009;42(2):377.
6. Sakles JC, Chiu S, Mosier J, et al. The importance of first pass success when performing orotracheal intubation in the emergency department. Acad Emerg Med. 2013;20(1):71-78.
7. Montalbano A, Lee B. Organization for urgent care health (OUCH): 2016 data. In: Pediatric Urgent Care Conference. Orlando: PM Pediatrics; 2018:Poster.
8. Yuknis ML, Weinstein E, Maxey H, et al. Frequency of pediatric emergencies in ambulatory practices. Pediatrics. 2018;142(2).
9. Ekezie J, Garthe C, Stanley R. Management of adult patients in the pediatric emergency department. Pediatr Clin North Am. 2018;65(6):1167-1190.
10. Samuels-Kalow M, Neuman MI, Rodean J, et al. The care of adult patients in pediatric emergency departments. Acad Pediatr. 2019;19(8):942-947.
11. Bourgeois FT, Shannon MW. Adult patient visits to children’s hospital emergency departments. Pediatrics. 2003;111(6 I):1268-1272.
12. Conners G, Committee on Pediatric Emergency Medicine. Pediatric Care Recommendations for Freestanding Urgent Care Facilities. Pediatrics. 2014;133(5):950-953.
Author affiliations: Amanda Montalbano, MD MPH FAAP, Division of Urgent Care, Children’s Mercy Kansas City; University of Missouri-Kansas City School of Medicine. Brian Lee, PhD MPH, Division of Health Services Research, Children’s Mercy Kansas City, Kansas City, MO. The authors have no relevant financial relationships with any commercial interests