
Urgent message: Management of face and scalp lacerations requires an appreciation of the unique anatomy, sound repair technique, and consideration of patient expectations for cosmesis.
TOYIN FAPOHUNDA-ADEKOLA MD, MBA
Lacerations of the scalp and face are commonly seen in the urgent care setting. While these injuries can cause anxiety for both patient and practitioner, the basic tenets and techniques for repair are already well known. Following a systematic approach and appreciating the unique anatomic considerations of the face will allow the urgent care practitioner to manage these wounds confidently and with optimal results. In addition to applying a sound technical approach to repair, understanding and responding to patient expectations and concerns are an important part of the evaluation and management of these injuries. Because disfiguring facial lacerations can cause significant emotional and psychological problems, long-term cosmesis must be a central component of decision making around management.
In this two-part series, we will review the approach to the face and scalp wounds most commonly seen in the urgent care setting. Anatomic considerations that influence the evaluation and management of these injuries also will be explored, as will identification of the steps necessary for an optimal repair.
General Approach
The objectives of laceration care are avoidance of infection and achievement of a practical and cosmetically acceptable scar. Lacerations of the face and scalp may involve blood loss, change in mental status or choking hazards. Therefore, initial manage ment must include assessment of stability and hemo dynamics, and attention to the ABC guidelines (i.e., Airway, Breathing and Circulation). Prior to treatment, a thorough patient history is necessary, with meticulous attention paid to factors that could adversely affect wound healing.

Anatomical Considerations
A basic appreciation of anatomy and the neurovascular supply of the face is critical prior to any discussion about evaluation and management of lacerations. Facial lacerations often include traumatic injuries to nerves and vessels that can have significant impact on healing, cosmesis and neurologic function. In addition, repair of these injuries requires an intimate knowledge of anatomy and cosmesis to achieve optimal results. Finally, because use of regional anesthesia is an important part of successful repair of the delicate tissues of the face and scalp, an appreciation of cranial nerve anatomy is paramount.
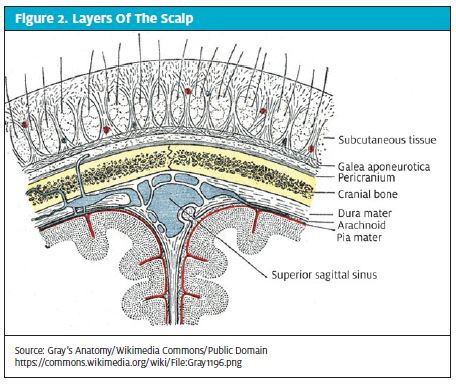
Anatomically, the scalp extends anteriorly from the supraorbital ridges to the external occipital protuberance posteriorly. Laterally, the boundaries are to the temporal lines. The scalp is composed of five layers: The skin (epidermis and dermis), the dense superficial fascia (fibro-fatty tissues), the galea aponeurotica, loose areolar connective tissue, and the pericranium or periosteum.
Within the dense superficial layer lies a rich supply of venous and arterial blood vessels. These vessels do not retract on laceration, which is important to note because any superficial laceration therefore has the potential to result in significant bleeding with hypovolemia and hypotension.
Most of the sensation in the face is provided by cranial nerve V (trigeminal), which has three major divisions: ophthalmic, maxillary, and mandibular. The ophthalmic division (V1) provides sensation to the upper third of the face, including the eyes and the nose down to the tip. The maxillary division (V2) provides sensation to the midface through the infraorbital nerve. The mandibular division (V3) supplies sensation to the lower third of the face.
Important muscles of the face include the muscles of facial expression that are innervated by cranial nerve VII (facial nerve), which travels through a narrow canal within the temporal bone. Facial fractures often are associated with injury to this nerve. The muscles of chewing are innervated by the fifth nerve, the trigeminal nerve, which controls jaw movement and nerves IX, and X (glossopharyngeal and vagus respectively), which control palatal movement.
Scalp Lacerations
Initial assessment of a scalp injury should include a rapid evaluation for potentially life-threatening situations, starting with evaluation of the ABCs to determine a patient’s stability. Pertinent history questions include the mechanism of injury and associated symptoms. Special attention should be paid to inquiring about symptoms associated with more significant head injury or concussion. Changes in mental status, coordination, speech, and behavior all should be assessed and risk of a co-existing c-spine injury should be assessed by evaluating for neck pain, step offs, weakness, paresthesias, and numbness. The possibility of a foreign body should be investigated when questioning a patient about the mechanism of injury. All of a patient’s prescribed medications should be reviewed for possible adverse reactions that may have contributed to the injury or that may impact healing. Recreational drug and alcohol use also should be assessed.
A methodical examination is key for any patient with a scalp injury. A thorough scalp examination should look to rule out signs of increased intracranial pressure (ICP) such as nausea, vomiting, fixed dilated or nonreactive pupils and altered mental status. For most scalp lacerations, initial management consists of applying direct pressure to the wound for 15 minutes with or without lidocaine plus epinephrine to achieve hemostasis. The presence of profuse bleeding or hematomas warrants inquiry about hematologic pathology (i.e., hemophilia and other factor deficiencies).
Appropriate lighting and control of bleeding are important to ensure that any foreign bodies can be identified. If the situation allows, a quick evaluation for concussion can also be conducted with rapid evaluation tools such as the Sport Concussion Assessment Tool (SCAT), which gives a quick neurologic evaluation.
During the examination, characteristics of the laceration should be noted, including the time of injury and the shape, length and, most importantly, the depth of the wound. The time of injury is important because laceration repair by primary closure is time dependent. Wounds healed by secondary intention are at increased risk of scarring. Involvement of the galea should be noted because it necessitates repair to prevent deformity.
Indications for imaging
Neuro imaging is an important consideration in head trauma and, if available, can be used in the urgent care setting for patients deemed stable and without risk of a co-existing c-spine injury. A computed tomography (CT) scan is warranted for patients who sustain their injuries from falls from height, blunt force trauma or situations related to drugs and alcohol. Plain films are no longer favored for evaluation of face and scalp trauma. Imaging to rule out intracranial injury also is warranted in cases involving exposure of bone. If foreign bodies are a possibility, plain radiographs can be used to detect radiopaque objects such as glass, whereas ultrasound can detect non-radiopaque materials.
Repair preparation and technique
Although wound irrigation is a common practice in laceration repair, research shows that with the rich supply of blood to the scalp, wound infections are rare. Therefore, for clean, non-contaminated scalp wounds, irrigation before primary closure does not change the rate of infection or cosmetic appearance.1
Anesthesia for scalp repair can be achieved using lidocaine with epinephrine (excluding the nose, eyelids and ears). (Epinephrine is included to provide additional hemostasis, as needed.) Although hair is seen by some as a contaminant, hair removal before closure is only called for in situations where the presence of the hair complicates the laying or knotting of the suture.2 Hair can be easily cleaned with the same bactericidal solution used for the laceration.
For repair of most simple scalp lacerations, staples can be used and they have the benefit of being faster and less expensive than, and yielding results similar to those for sutures (Figure 1).
In the other hand, staples should NOT be used for lacerations involving the galea. An anchoring point for the frontalis muscle, the galea must be repaired separately to prevent deformities and asymmetry in facial expression (Figure 2). Repair can be achieved with 3.0 or 4.0 absorbable sutures (i.e. Vicryl, Monocryl etc.) using a single interrupted technique. Besides preserving muscle use, galeal repairs prevent subgaleal infections and the spread of infections throughout the scalp.
Less frequently used but equally effective for closing scalp wounds is the Hair Apposition Technique (HAT). This technique is best for hemostatic wounds that are less than 10 cm long and when the scalp hair is longer than 3 cm. With HAT, opposing hair strands are brought together with a simple twist and are locked with a drop of tissue adhesive.3
Empiric antibiotics are not usually indicated for scalp lacerations but are warranted for bites (animal and human) and excessively contaminated lacerations. All adults with scalp lacerations should receive tetanus (Td) or the Tetanus, diphtheria, pertussis (Tdap) vaccination if there is uncertainty about their vaccination status. Scalp lacerations that do not require pressure dressings can be left open to air and washed gently with soap and water after 24 to 48 hours. Staples or non-absorbable sutures can be removed in 5 to 7 days.
Forehead Lacerations
Lacerations of the forehead are common in both children and adults and have the potential to arouse a fair bit of anxiety in patients because of the possibility of scarring in a highly visible area. The tension lines on the forehead are discussed in detail here because an understanding of them is necessary to ensure a good cosmetic result.
Tension lines
Relaxed skin tension lines (RSTLs) generally run at right angles to the direction of the underlying musculature (Figure 3). Repair of lacerations in the direction of the tension can help minimize scarring and produce the best aesthetic results.4 A horizontal laceration of the forehead, for example, will be under minimal tension because it is parallel to tension lines, whereas a vertical laceration will be more gaping and difficult to repair and will heal with more scarring. Research shows that repair according to RSTLs is the key to less scarring and actually is more important than the repair technique.5 Nevertheless, it is important for urgent care practitioners to counsel patients about expectations for surgical outcomes in cases when scarring is more likely. Revision of scars by a plastic surgeon is always an option, but if there is any concern about appearance, early referral and primary closure with cosmetic techniques should be considered.
Repair Preparation and Technique
The first step in preparation for repair of a forehead laceration is to inspect the wound carefully for foreign bodies so as to prevent traumatic tattooing, a phenomenon that occurs when foreign bodies are retained within tissue. Anesthesia for forehead lacerations is dependent on wound size. For small lacerations, 1% lidocaine or LET (lidocaine 4%, epinephrine 0.1%, and tetracaine 0.5%) can be used locally, but if the injury covers most of the forehead, a regional block with lidocaine) may be appropriate.
For forehead lacerations, use of adhesives such as octylcyanoacrylate (Dermabond® and Histocryl®) often is a consideration. It is imperative, however, that urgent care providers have a careful understanding of the conditions for use of these products and are experienced with proper application techniques. (For an in-depth article on adhesives, please view Using Tissue Adhesives in Urgent Care in the December 2013 edition of JUCM.) In order to promote optimal cosmesis with adhesives, hemostasis must be completed and perfect alignment of the edges must be ensured. Other important considerations include prevention of adhesive drips, particularly into the eyes and lips. In situations where the laceration is irregular, gaping, or approximation of the edges cannot be guaranteed, sutures should be exclusively used. The skin on the face is some of the thinnest on the human body, and thus, prone to tears and dimpling, risks which can be minimized by choosing the smallest size suture adequate for the job. In most cases, 6.0 suture (monofilament or rapid absorb) in a technique involving multiple small “bites” will mitigate the risk.
Home care and follow up
For forehead lacerations, a dressing usually is not required. Patients should be counseled to keep the site clean by gently washing (but not scrubbing) their face twice a day and to apply topical antibiotics thereafter.


Eyelid and Eyebrow Lacerations
Eyebrow lacerations are most often caused by blunt trauma to the supraorbital area. For any laceration involving the eye (brow, lid etc.), a full and careful examination of the eye is required before repair is performed. The examination should include assessment of visual acuity and extraoccular movement, ophthalmic inspection for hyphemas, and fluorescein stain for corneal abrasions.
Lacerations involving the medial canthus or the medial third of the upper or lower eyelid should raise suspicion for damage to the canalicular drainage system and require assessment by ophthalmology. Although canalicular injuries require specialty consultation, they can be repaired up to 48 hours after the injury, should that be necessary (weekends/after hours). Patching of the eye may be necessary to keep the wound clean and dry pending follow-up.
With injury to the eyebrow and eyelid, it is important to look for clinical clues that may raise suspicion of deeper injuries. Copious tears, for example, may indicate injury to the tear duct, whereas an acute case of strabismus post-injury indicates injury to the medial palpebral ligament. In addition, any laceration to the eye that results in protrusion of fatty tissue from the wound should raise concern for a torn orbital septum, and acute ptosis post injury may indicate injury to the levator palpebrae superioris. Urgent care providers should also have a low threshold for obtaining a CT scan to inspect the orbits and to rule out fractures when periorbital edema and ecchymosis are present.
If the examination reveals or raises suspicion of a penetrating globe injury (Table 1), the examination should be stopped and the patient should be referred immediately to an ophthalmologist or transferred to the emergency department. DO NOT manipulate the eye, apply any pressure to the globe, patch the eye or measure intraocular pressure.
Repair preparation and technique
For lacerations to the eyebrow, the eyebrow hair should never be shaved because regrowth cannot be guaranteed. Sutures are not necessary for lacerations shorter than 0.25 cm that are located above or below the eyebrow; steri-strips or a topical triple antibiotic (i.e. neomycin) can be applied.1
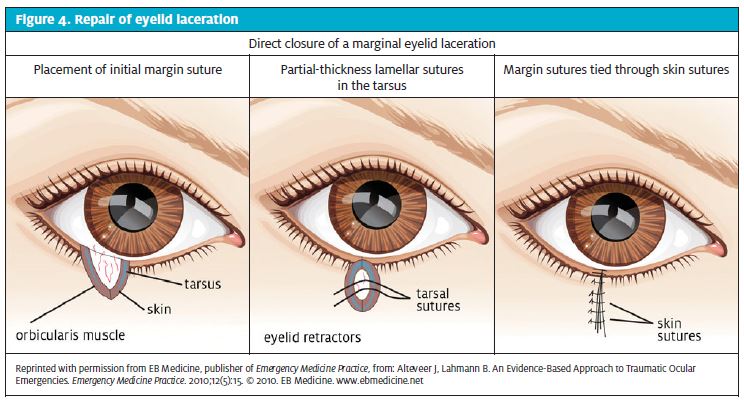
When sutures are necessary, the eyebrow should be sufficiently irrigated with normal saline (ensuring that the eye is protected) and the eyebrow anesthetized with LET or lidocaine with or without epinephrine. For eyelid lacerations, lidocaine alone should be used because epinephrine is contraindicated. Absorbable (6.0) or permanent sutures (6.0 or 7.0 nylon) are acceptable for suturing. For deep lacerations, each tissue layer may need to be repaired individually and care should be taken to realign the wound edges anatomically (Figure 4).
This can be achieved by suturing the superior and inferior margins first. When suturing the eyelids, special care must be exercised to avoid piercing the needle through-and-through the eyelid. Furthermore, never apply pressure on the globe of the eye while repairing eyelid wounds.
Adhesives for eyebrow lacerations
Given the ease of use and pain-free attributes of skin adhesives, urgent care providers may be tempted to use them for repair of eyebrow lacerations. With standard, low-viscosity octylcyanoacrylate (OCA) skin adhesives, there is a risk of migration, and great care and significant skill are needed to avoid accidental tarsorrhaphy. High- viscosity OCA has been associated with dramatically less migration than are lowerviscosity products.6 Even with high-viscosity adhesives, great care should be exercised around the eye. For eyelid lacerations, adhesives should be avoided entirely.
After care
For eyebrow or eyelid lacerations, after care includes provision of tetanus prophylaxis, referral and follow-up as needed, and clear home care instructions. The laceration site should be gently cleaned twice a day; topical antibiotics also can be applied. Sutures can be removed in 3 to 5 days and steri-strips applied as necessary.
Conclusion
When presented with a patient who has lacerations of the face or scalp, an urgent care provider’s initial concerns focus on eliminating choking hazards, controlling blood loss, and preventing infection. Decision-making about wound management also must take into consideration long-term cosmesis because of the potential for disfigurement. To help ensure the best possible outcome for patients with injuries to the scalp, forehead, eyelids, or eyebrows, an understanding of the anatomy and use of appropriate repair techniques, as described here, is critical. Part 2 of this article, in next month’s issue, will examine the approach to lacerations of the ear, nose, cheek, lips, and tongue.
Reference
- Ehrardt CR. Eyebrow Laceration Repair. Ambulatory Care Procedures for the Nurse Practitioner. 2003 pp 326.Anderson L, Kahnberg KM, Pogrel P, Eds. Oral and maxillofacial surgery. John Wiley & Sons, 2012.
- Trott AT. Wounds and lacerations: emergency care and closure. Elsevier Health Sciences. 2012.
- Hock Mo, Ooi SB, Saw SM, et al. A randomized controlled trial comparing the hair apposition technique with tissue glue to standard suturing in scalp lacerations (HAT study). Ann Emerg Med. 2002;40(1):19-26.
- Anderson L. Kahnberg KM, Pogrel P, Eds. Oral and maxillofacial surgery. John Wiley & Sons, 2012.
- Borges AF. Relaxed skin tension lines. Dermatol Clin. 1989;7(1):169.
- Singer AJ, Giordano P, Fitch JL, et al. Evaluation of a new high-viscosity octylcyanoacrylate tissue adhesive for laceration repair: a randomized clinical trial. Acad Emerg Med. 2003;10(10):1134-1137.