
Urgent message: Lower extremity injuries are very common in adolescent athletes. Urgent care providers must remember that shin pain is not always simply shin splints.
CHRISTOPHER TANGEN, DO, and RYAN SHILIAN, DO
Also known as medial tibial stress syndrome, shin splints are described as the painful inflammation of the tibial periosteum, which is generally caused by repetitive physical activity.1 Repetitive injuries can cause incomplete fractures, or microfractures, of the tibia. These tibial stress reactions can predispose the bone to acute fractures.
Case Presentation
A 15-year-old high school athlete fell directly onto his right shin while practicing football. He experienced severe pain and was transported off the practice field, where he was immediately evaluated by his athletic trainer. At that time, the pertinent finding was mid-shaft tibial tenderness to palpation. The athlete was sent home on crutches, and it was recommended that he rest and ice the area and also use ibuprofen for pain. His pain persisted the next day, and he sought treatment in an urgent care center. At that time, he was unable to ambulate because of severe pain, so he used a wheelchair.
Findings on his medical history, surgical history, social history, and family history were unremarkable. He had no allergies, and he was not taking any other medications.
Physical Examination
Evaluation of the patient showed the following:
- Temperature: 98.7°F (37°C)
- Pulse: 63 beats/min
- Blood pressure: 127/83 mm Hg
- Oxygen saturation: 100%
On physical examination, the patient was found to be in mild discomfort but was fully alert. No abnormal findings were noted on his cardiovascular and respiratory examinations. Examination of his right lower extremity revealed severe tenderness and also edema overlying the mid-shaft of the right tibia. A tibia-fibula squeeze test of his right leg elicited pain. The leg was neurovascularly intact.
Diagnosis
Acute nondisplaced fracture of the right mid-tibial shaft.
Resolution
The patient’s leg was stabilized in a long leg splint, and he was given crutches and referred to an orthopedic surgeon. Acetaminophen-codeine oral tablets, 300/30 mg, were prescribed for pain.
After orthopedic evaluation within 3 days, the patient was given a long leg cast and was instructed to continue avoiding bearing weight on his right leg.
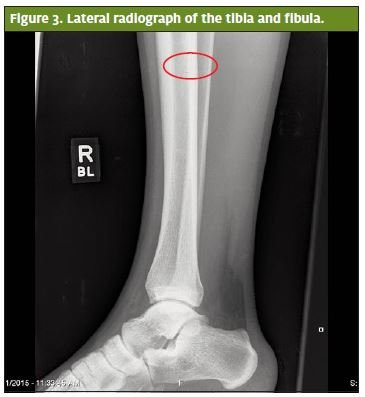
Anteroposterior (Figure 1) and lateral (Figures 2 and 3) tibia and fibula plain film radiographs were ordered. These revealed an acute nondisplaced fracture of the mid-diaphysis of the right tibia (Figures 1, 2, and 3).
 Discussion
Discussion
Medical History
Shin splints are considered to exist on a spectrum of tibia injuries that includes simple overuse injuries from repetitive stress, stress fractures, and acute fractures.1 Lack of conditioning, imbalances in muscle training, and trauma are factors that lead to worsening injuries. Patients with shin splints will present with a history of diffuse shin pain for up to several weeks. The specific time patients experience pain is an important piece of the medical history. Athletes with shin splints will often report that their pain is worse right after participating in sports, but they will notice their pain with every step they take if they have acute or stress fractures.
Physical Examination
Shin splints generally present with pain along a portion or majority of the tibial border, often with diffuse tenderness. Recent stress fractures or acute tibial fractures will present with specific tenderness to palpation and often have associated soft tissue swelling at the area of the fracture and pain with weight-bearing.3
With acute tibial shaft fractures, patients are unable to bear weight because of severe pain and edema.3 Pain, pulselessness, pallor, paresthesias, and poikilothermia can be signs of compartment syndrome. Indications for emergency orthopedic referral within 6 hours include compartment syndrome, neurovascular injury, open tibial shaft fractures, and the presence of concurrent dislocation of the knee or ankle.3
Diagnostic Testing
Plain film radiographs are the first imaging step in the evaluation of a suspected tibial fracture. If further injury is suspected, computed tomography imaging and ultrasound can be considered for a complicated fracture and vascular etiology, respectively.
Treatment
General
General treatment of shin splints includes ice, rest, stretching, avoidance of repetitive injury, physical therapy, and nonsteroidal anti-inflammatory drugs. Athletes can attempt to prevent shin splints and stress fractures by running on softer surfaces, performing daily hamstring and calf stretches, ensuring proper fit of their shoes, and gradually increasing repetitive stress activities.
Tibial Shaft Fractures
Tibial shaft fractures that are nondisplaced and that are not comminuted can be comfortably treated by primary- care physicians and urgent care providers. Initial treatment of closed tibial shaft fractures involves immobilization in a long leg posterior splint, applied with the knee held in 10° to 20° of flexion. If a patient is having persistent pain after splint placement, it can be a sign of limb ischemia or compartment syndrome.2
Long-Term Course and Complications
It is important for the patient to avoid weight-bearing on the affected extremity for 1 to 2 weeks. Then as soon as the edema subsides (in 2–3 weeks), the cast is changed to better immobilize the affected area. It usually takes an additional 1 to 4 weeks for evidence of satisfactory healing to be detectable on radiographs. At this point, the cast can be exchanged with a walking cast boot or a short leg walking cast. It normally takes 10 to 14 weeks for non – displaced fractures to heal.3
Potential long-term complications of immobilization of a nondisplaced tibial fracture include nonunion, malunion, complex regional pain syndrome, joint stiffness, infection, and refracture.3
 Red Flags
Red Flags
The limb must be examined for palpable bony deformities, signs of infection, compartment syndrome (the five P’s: poikilothermia, paresthesia, paralysis, pallor, and pain), and other vascular injury, all of which require immediate treatment.4 Cyclical pain, fever, and unexplained weight loss can be clues in the medical history for consideration of fractures from primary or secondary bone tumors, or from infectious etiologies such as osteomyelitis.
Take-Home Points
School and recreational sport seasons bring many patients to urgent care centers for various lower extremity complaints, and the majority of athletes with shin pain have shin splints. Primary-care physicians and sports medicine specialists are appropriate specialists for recommendations for follow-up and referral in cases of shin splints that do not heal after initial treatment.
However, because not all shin pain is caused by shin splints, obtaining a thorough medical history and conducting a detailed physical examination, along with interpreting plain films, may lead to discovery of more serious injuries such as nondisplaced tibial shaft fractures.
References
- Medial tibial stress syndrome (shin splints). In: Safran A, Zachazewski J, Stone DA, eds. Instructions for Sports Medicine Patients. 2nd edition. Philadelphia, PA: Saunders; 2012: 617–620.
- Pallin DJ. Knee and lower leg. In: Marx J, Hockberger R, Walls R, ed. Rosen’s Emergency Medicine: Concepts and Clinical Practice, 8th edition. Philadelpha, PA: Saunders; 2013: 731–744.e1.
- Patellar, tibial, and fibular fractures. In: Eiff MP, Hatch RL, eds. Fracture Management for Primary Care, 3rd edition. Philadelphia, PA: Saunders; 2011: 245.
- Rudloff MI. Fractures of the lower extremity. In: Canale ST, Beaty JH, eds. Campbell’s Operative Orthopaedics, 12th edition. Philadelphia, PA: Mosby; 2013: 2617–2724.