Urgent message: Companies like Apple and Nordstrom have raised the quality of customer experience to an art form, one that urgent cares would do well to emulate.
ALAN A. AYERS, MBA, MACC, Experity
Introduction
Urgent care is positioned as a consumer-focused delivery channel for low-acuity medical services differentiated from hospital emergency departments and primary care practices by retail-facing
locations, extended evening and weekend hours, and walk-in convenience. As with airlines, restaurants, and other service businesses, urgent care thrives on repeat visits and positive word of mouth from satisfied patients. Fostering patient loyalty requires an urgent care center to not only resolve the medical problem that is the reason for the patient’s visit efficiently and courteously but to do so in a way that creates a positive emotional connection with the patient.
Focus on the Patient Experience
When was the last time you had a negative customer service encounter? Do you think the investors, management, and employees of the operation deliberately set out to disappoint you? If you ask most front- line employees whether they deliver “good service,” their answer should be a unanimous Yes. The problem is that service providers and consumers often have different perspectives on what constitutes good service. For example, an airline may arrive on schedule and without a safety incident—successfully delivering its “service”—but passengers who encounter drab terminals, long lines, bitter staff, and cramped seats will hardly “rave” about the experience. Merely delivering a “service” makes for a commodity provider that, by definition, has no brand loyalty and no competitive advantage.
If patients perceive all urgent care centers as equal in their ability to treat minor medical conditions, they will migrate to providers who offer the best overall experience. This means an urgent care operator who defines good service only in terms of clinical out- comes will rarely see the profitability and growth of a center that demonstrates passion, ingenuity, and authenticity in every detail of a patient visit. So how do you practice good medicine and offer good service from a patient perspective?
Phase One: Clarify Who You Are and Who You Hope to Become
When an urgent care operator realizes the need to improve the patient experience, he typically starts looking to implement quick and easy fixes. But rarely do solutions that address no specific problem make an impact, particularly when the center’s strategies priorities are undermining the patient experience.
Consider how an urgent care operator focused on maximizing daily profit margin (as opposed to growing net profits) can achieve his goals by short-staffing the center, limiting hours, and spending capital only when absolutely necessary. The result is a cost-driven culture that attracts the lowest paid workers to a shoddy facility with poorly maintained equipment, which, over time, patients will shun, given better choices. No successful business has ever cost-cut itself to prosperity. Growth requires investment in the people and infrastructure that deliver the service patients expect. There are no sufficient superficial fixes to impact an operation that, by design, sees the patient experience as an expense to be eliminated.
Undifferentiated commodity providers focus on controlling cost, but leading consumer brands invest millions to grow revenue by developing an emotional connection with consumers. Viewed as “cool,” “real,” “unique,” “original,” or “edgy,” they integrate products, people, processes, systems, and environments to create an experience that’s fundamentally better than competitors. Short of inventing something completely new, an urgent care operator can borrow elements of leading consumer brands to create a culture that is aspirational yet achievable. The starting place is to identify one or two service cultures that relate to consumers exceptionally well. Consider whether your center strives for the brand attributes of, for example, Apple vs Hewlett-Packard, Starbucks vs McDonald’s, Southwest Airlines vs American Airlines, Ritz Carlton vs Holiday Inn, or Nordstrom vs Walmart.
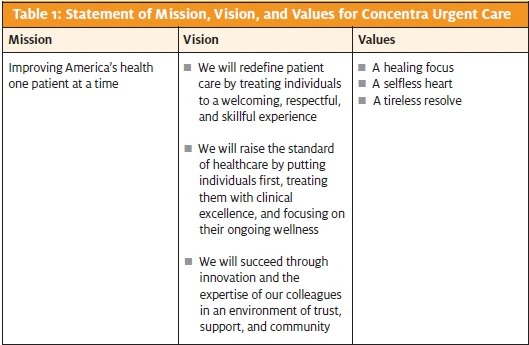
Once you identify brands that represent how you’d like patients to view your center, your “desired” state manifests in the form of a mission, vision, and values statement. Consider the mission, vision, and values statement for Dallas, Texas-based Concentra Urgent Care, with over 310 centers in 40 states (Table 1). It describes why the operation exists, what it intends to accomplish, and the values that direct its activities.
A center’s mission, vision, and values don’t need to reflect the reality of today’s operation. More often, they are guiding principles that point to where an organization strives to be in the future. So if you envision your front-office staff giving repeat patients a warm welcome like a Starbucks barista—but today your staff is better described as “crisp” and “efficient”—expectations can be set as to who the staff will become.
Measure the Patient Experience
Once the center’s service and cultural attributes are defined, a measurement system is needed to assess how well the center is delivering on patient expectations and provide evidence that improvement initiatives are working. Otherwise, “proud” providers and staff may persist in behaviors they believe constitute good service but which have no impact on patient perceptions. A patient experience survey—elicited by in-center comment cards or a mail, telephone, or email survey (or a combination of these)—provides quantitative and qualitative data for evaluating operations:
- Quantitative data can be compiled from numerical assessments: surveys in which questions are answered on a scale of 1 to 10, with 1 being poor and 10 excellent. Questions should include patient satisfaction with the visit, whether a patient would recommend the center to friends/family, and satisfaction with staff communication of wait times. Responses are then tracked over time to identify trends. Quantitative survey data should be regularly posted in an area visible to providers and staff. Tracking progress spurs continuous quality improvement.
- Qualitative data consists of patient compliments, complaints, and suggestions for improvement all of which require a response from the urgent care operator. Qualitative feedback should be shared in staff meetings to recognize individuals delivering outstanding service, explore ways to implement patient suggestions, and devise remediation plans for the complaints.
An urgent care operator should strive for continual improvement. The reason for the patient’s complaints should be immediately resolved while also assessing the root causes. For long-term planning, the real value of patient feedback is the insight it provides into the patient’s mind. What one patient sees and speaks out about is silently in the thoughts of hundreds of other patients. So the answer to the question, What does good service look like?, can typically be found in patient comments.
The challenge, of course, is that patient intentions are not always clear. Consider the following two patient “complaints” written on a visit comment card:
- “The exam table cover had duct tape on it.”
- “The front office staff was slow and rude.”
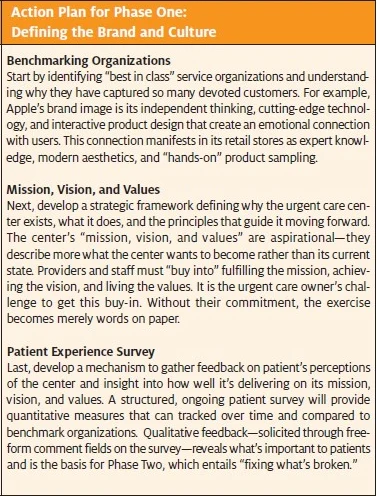
The first complaint is easily resolved by repairing upholstery. But the second complaint not only begs the question, What constitutes slow and rude?, but the resolution involves the complex interdependencies of hiring, training, operating procedures, and systems (see Action Plan for Phase One: Defining the Brand and Culture).
Phase Two: Identify and Resolve Barriers to Good Service
Urgent care is a “people” business not only are people needed to deliver clinical services, but people are the largest expense on the center’s profit-and-loss statement. Therefore, it’s logical that the biggest barriers to good service involve people. If there are providers or staff who actively undermine the center’s mission, vision, and values—or who are simply incapable of delivering the desired service levels—then seriously consider letting them go. They are hurting the business and will stand in the way of any meaningful change. When back filling their roles, interviewing for attitude, personality, and behavioral traits (in addition to technical competence) can help improve the odds that new team members are willing and able to perform as expected. Once the right team is in place, “fixing what’s broken” entails setting standards based on patient expectations and then educating providers and staff.
Service standards define the experience that everyone in the urgent care center is responsible for delivering. They affect all aspects of an operation, including which programs are shown on the television in the waiting room, how the telephone is answered, and what documentation is provided to a patient at discharge. Service standards should be specific, detailed, and baked into the center’s written policies and procedures. There should also be a mechanism for managers to hold staff accountable for their execution. To this end, service standards may be:
Descriptive—such as “every exam room should have no fewer than three magazines, in good repair, with no torn pages, water damage, or stains, with each issue current, no more than 30 days old, with separate titles appealing to women, children, and general interest”in which case an operator may randomly spot- check exam rooms to assure compliance
- Measured—such as “time elapsed from sign-in to discharge should not exceed 60 minutes”in which case the opera- tor utilizes billing system data to report how consistently providers and staff meet the standard
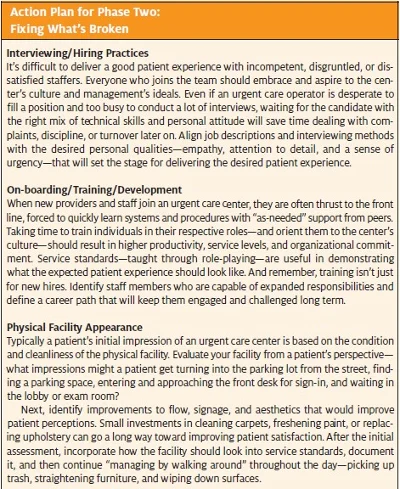
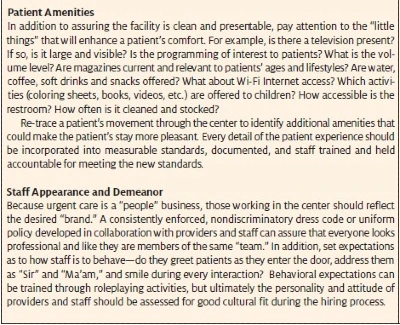
Service standards are effective insofar as they align with the center’s mission, vision, and values; are developed in collaboration with providers and staff; and are frequently communicated so that everyone (including patients) knows what to expect. To assure consistency in execution, training is essential. Photographs, testimonials, and role- playing activities illustrating “good” and “bad” service can help orient providers and staff to the patient’s perspective. When shortcomings are revealed, they should be pointed out immediately so staff can take corrective action and be more aware and sensitive going forward (see Action Plan for Phase Two: Fixing What’s Broken).
Phase Three: Align and Focus the Operation in Execution
Buzzwords like “empowered” and “engaged” are commonly used to describe teams who deliver a consistently high level of service— resulting in benchmark brands like Starbucks and Nordstrom—but rarely can urgent care providers and staff, who struggle just to keep the patient flow moving, change the quality of service entirely on their own. Even the most committed teams require a leader to set priorities, allocate resources, remove barriers, and instill measures to hold team members accountable for positive results. Thus, “Phase Three” entails changing management methods to leverage the front-line knowledge and creative instincts of providers and staff by aligning activities and incentives with operational priorities.
For example, an urgent care operator identifies that long patient waits are adversely impacting patient satisfaction. The center team meets to identify how every- one’s role affects wait times. Collaboratively, the team comes up with a plan of action—a commitment of each individual to change his/her way of doing some- thing. Accountability comes by setting a measurable goal, such as: “Reduce average length of stay by 10 minutes by November 1.” Incentives (such as a paid vacation day or a cash bonus) are put in place if the goal is met or exceeded. Management provides regular reports on the team’s progress. Everyone works together to affect change until the goal is met, at which point the changes are permanently adopted into policies and procedures and the process repeats for the next priority.
Develop Authentic Relationships
Engaging the front line to make an impact on the patient experience requires the urgent care operator to abandon pretense and hidden agendas in favor an authentic, transparent environment where everyone is working toward the same purpose. While slogans and buzzwords may have been useful in orienting employ- ees in Phases One and Two, “bottom-up” management requires employees who are fully empowered to do what’s necessary to please the patient.
But just because an employee is “empowered” doesn’t mean he or she is “engaged” in delivering an excellent patient experience. In fact, many employees see work as their primary social outlet and are engaged with one another in “solidarity” against management and patients. Many managers believe that compensation is the key to motivating such employees, but staff that is focused on a paycheck will do the minimum, play games, evade problems, and undermine change. In the short term, they may be motivated by incentives such as receiving a bonus or evading disciplinary action, but over the long term, consistent execution requires people to act from their hearts and minds. Recognition or praise for exhibiting the “right” behaviors, the ability to engage in interesting and challenging work, and training and development with an eye toward promotion do more to motivate employees than a mere salary or bonus.
Authoritarian, punitive, top-down leadership will not work when an urgent care operator needs providers and staff to take personal responsibility for the patient experience. Ultimately, “winning over” employees requires an urgent care operator to understand and align employees’ long-term interests with that of owners and management. The most engaged employees find a sense of personal meaning in their work and in the center’s mission, vision, and values. “Inspired” employees who feel personal responsibility for creating good patient experiences should be more productive, more creative, demonstrate greater integrity, and work better in team environments than those who are merely doing a “job.”
Anticipate Change
The American railroad industry got pummeled because of competition from trucks, airplanes, and automobiles. The problem was that railroads saw themselves as being in the “train” rather than the “transportation” business, and as customer needs evolved, railroads were regarded as rigid and slow. Likewise, urgent care centers shouldn’t see themselves as being in the business of treating “low-acuity medical conditions” but rather of treating patients well.
Leading service companies not only view themselves in terms of meeting a customer need, their technology and procedures anticipate and adapt to change. Take Wells Fargo, which, over the course of 150 years, has migrated from a stagecoach courier service, to a coast- to-coast bank branch network, to offering Internet and mobile “financial management tools” available wher- ever a consumer might be. To avoid being left behind when new technologies like online medical records and telemedicine become more commonplace, urgent care centers should likewise evolve.
For urgent care operators, technology that improves the patient experience can be a differentiator. For example, Internet pre-registration and scheduling reduce patient waits, improve billing accuracy, and free center staff to focus on the care provided to patients. The task for urgent care operators is to identify creative uses for technology and make the investments required (see Action Plan for Phase Three: Consistent Execution of Phase 1 and 2 Initiatives on page 33).
Conclusion
“Superior service” has been the mantra of consumer-facing organizations for years, which means the general public has many preconceived notions of what an urgent care encounter should and should not entail. An urgent care center delivering an experience that falls short of patient expectations—regardless of the quality of clinical outcomes—will find revenue growth slow and hard to come by. By progressing through the three phases outlined, however, an urgent care operator can identify what’s important to patients, engage providers and staff around a common purpose, devise measures, and ultimately hold the team accountable for anticipating and responding to patients’ evolving needs
