Published on
Urgent Message: Chronic cough has a distinct differential diagnosis in different age groups. A cough lasting longer than 4 weeks in children and adolescents should prompt revision of the differential diagnosis to reduce delays in diagnosing serious etiologies.
Daniel Moscato, MS, PA-C; Joshua W. Russell, MD
Citation: Moscato D, Russell JW. Uncovering the Unexpected: A Case of Chronic Cough in an Adolescent with an Unusual Etiology. J Urgent Care Med. 2025; 19(4)23-26.
Key words: Pediatrics, cough, Hodgkin lymphoma
Abstract
Introduction: Cough is an exceedingly common pediatric chief complaint in urgent care (UC) settings and is most often attributable to an infectious cause. However, clinicians must refine and alter their differential diagnoses when the cough persists to ensure serious etiologies are diagnosed in a timely fashion.
Presentation: A 14-year-old girl presented to UC with cough for 6 weeks. She had multiple presentations to UC for these symptoms over prior weeks; a viral upper respiratory infection (URI) diagnosis was assigned at each preceding visit. Symptomatic therapies were recommended. She was prescribed a short course of systemic steroids, which resulted in mild and transient improvement.
Physical Examination: The patient’s vital signs were all normal and her physical examination was only remarkable for a persistent, dry cough. Auscultation of bilateral lungs revealed no adventitious lung sounds.
Diagnosis and Resolution: Due to the refractory and chronic nature of her cough, a chest x-ray (CXR) was obtained which revealed a mediastinal mass. The patient was referred to the emergency department (ED) for further specialist evaluation and management. She subsequently had a biopsy as an inpatient, which confirmed a diagnosis of Hodgkin lymphoma (HL).
Conclusion: The differential diagnosis for children with cough lasting >1 month is broad, and more serious etiologies, beyond URI, should be considered to ensure timely diagnosis and optimal outcomes.
Introduction
Cough is a common presenting symptom for pediatric UC visits. Of all cough etiologies, respiratory infection is the most frequent etiology and reason for antibiotic prescription in children.[1] Although the symptoms of respiratory infections typically resolve spontaneously over 7-10 days, cough persists not infrequently for up to 3-4 weeks.[2] The prevalence of chronic cough without respiratory tract infection increases with age in the pediatric population.[3] In children 14 years and younger, a cough is defined as chronic if it persists beyond 4 weeks. The leading causes of chronic cough in children are asthma, bacterial infections (eg, pertussis), chronic rhinosinusitis/upper airway cough syndrome, and gastroesophageal reflux disease (GERD).[4],[5] It is especially important, given the prevalence of cough as a chief complaint, to consider etiologies beyond respiratory infections, particularly during the seasonal respiratory infection periods.
Clinical Presentation
A 14-year-old girl presented to UC with a chief complaint of cough for 6 weeks. The visit presented was the 3rd UC visit during her illness. When the cough began, it was productive, however, at the time of the visit, the cough had become dry and was keeping her up at night. The patient had no associated fever, rash, headache, eye redness/discharge, nasal congestion, earache, sore throat, wheezing, dyspnea, chest pain, reflux type symptoms, abdominal pain, nausea, vomiting, diarrhea, changes in urination, or changes in appetite.
At each of the prior UC visits, the patient was diagnosed with a viral URI and associated bronchitis. Symptomatic treatments were recommended initially, including over-the-counter and prescription cough suppressants. Given insufficient relief, she was subsequently treated with trials of short acting inhaled bronchodilator (ie, albuterol sulfate), an inhaled corticosteroid, and finally systemic corticosteroids. The patient’s parent reported that there was transient relief of the cough after the course of oral steroids, but the cough worsened again after stopping these. No imaging was performed at any of her prior visits.
The patient and parent denied that she had any significant past medical history. Specifically, they denied any known history of asthma or pneumonia. The patient denied any history of smoking/vaping as well.
Physical Exam Findings
On presentation to UC, the patient’s vital signs were all within normal limits. On examination, she seemed comfortable without signs of respiratory distress. The patient had a persistent, dry cough noted throughout the visit, which did seem somewhat worse when supine. On auscultation, there was good air movement throughout all lung fields without expiratory/inspiratory wheezing, crackles, rales, or rhonchi.
Patient/Parent Perspective
The parent expressed concerns about the chronicity and persistence of the patient’s cough, which she had never experienced before. The stated reason for the return visit was nominally to get a prescription for another course of oral steroids as that was the only thing that had helped, albeit transiently.
Medical Decision Making/Differential Diagnosis
The patient presented was a previously healthy, adolescent female with 6 weeks of dry cough. Her vital signs and physical exam were reassuring, and the only finding was a prominent, dry cough. She had negative influenza and SARS-CoV-2 viral testing at her prior visits.
Given her refractory and persistent symptoms despite multiple approaches to treatment, the differential diagnosis was broadened. Diagnoses considered included persistent infectious etiology (pneumonia), post-infectious hypersensitivity or bronchitis, new-onset asthma, upper airway cough syndrome, GERD, and upper airway compromise/mass effect. As there were no preceding URI symptoms, a benign lung exam, and poor response to anti-tussive agents, an infectious/post-infectious and/or upper airway etiology seemed less likely. Additionally, the patient experienced no relief from a trial of inhaled bronchodilator or steroid, which suggested reactive airways disease was also somewhat less likely. There were no abdominal symptoms, burping, association with certain foods or timing of eating, so GERD was also felt to be unlikely.
As the patient’s cough met the definition for “chronic” (ie, lasting >4 weeks), a CXR was ordered to screen for alternate diagnoses.
Urgent Care Management and Disposition
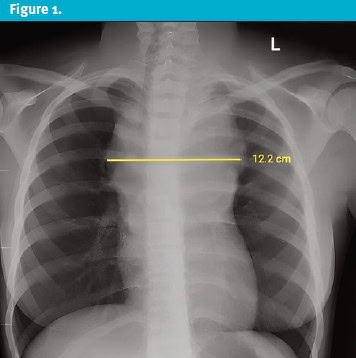
The CXR revealed a prominent, left-sided, soft tissue mass in the superior mediastinum with right tracheal deviation (Figure 1). Results were discussed with the patient’s caregiver, and the patient was subsequently referred to the ED for further specialist evaluation and management.
At 24-hour follow up, the patient had been admitted to the oncology unit at the local children’s hospital. She was admitted with a provisional diagnosis of lymphoma and high-dose steroids were started while awaiting biopsy results.
Final Diagnosis
The mediastinal mass was determined to be related to Hodgkin lymphoma, which was confirmed by biopsy.
Discussion
Cough is the most common presenting symptom in the pediatric population, especially during the respiratory viral infection season. Most acute coughs (ie, <4 weeks in duration) in children are related to viral/post-viral URIs and do not require further investigation.[6] Once a cough becomes chronic, investigations should include a thorough history, physical examination, CXR, and, when age-appropriate, spirometry (pre- and post-B2 agonist treatment).[7] With prudent consideration and further work-up, more severe causes for a chronic cough, such as the case patient’s final diagnosis of HL, can be identified in its earlier stages.
HL is one of the most common cancers in adolescents and accounts for 18% of all cancer diagnoses in children and young adults in the United States.[8] The incidence of HL follows a bimodal age distribution, peaking first during young adulthood and then again after 50 years of age; HL is very rare <5 years of age.8 Family history of HL is a significant risk factor with a reported 7-fold increased risk of HL in patients whose parent was afflicted and an 11-fold increased risk in patients <37 years with an affected sibling.[9]
Common presenting signs and symptoms of HL in children include lymphadenopathy, systemic complaints, and mediastinal mass. Most children with HL present with painless lymphadenopathy, commonly presenting as matted, firm masses of the cervical/supraclavicular or axillary regions.8 Up to 75% of children with HL will also have a mediastinal mass on CXR at the time of presentation; approximately 30% of such masses are greater than one-third the diameter of the intrathoracic cavity.8,[10] These “bulky” masses, as was present in this case, can cause compressive symptoms resulting in dysphagia, orthopnea, cough, stridor, or superior vena cava syndrome.10 Approximately 25% of patients will also develop systemic, or so-called “B” symptoms, such as fevers, unintentional weight loss (≥ 10% of body weight within 6 months of diagnosis), and night sweats.8
If concerning lymphadenopathy is detected, children and adolescents undergo an excisional lymph node biopsy for histologic diagnosis. Biopsy of HL demonstrates the “classic” finding of Hodgkin/Reed-Sternberg cells.8 Once the diagnosis of HL is confirmed, clinical staging, based on the Ann Arbor classification is performed for risk stratification. Stage is classified based on the quantity and location of lymph nodes involved in addition to the absence/presence of concomitant symptoms.8 While oncologists have made progress in the diagnosis and treatment of HL over time, survival rates, cancer-related quality-of-life, and long-term treatment-related morbidities continue remain largely unchanged.8 Proposed hypotheses for such gaps include age-related differences in disease and host biology, diagnosis delays, lower rates of clinical trial enrollment, treatment at facilities without young adult experience, and high rates of loss-to-follow up after achieving remission.8Across all risk groups, pediatric HL treatment regimens historically have utilized a combination of conventional chemotherapeutic agents including alkylators and anthracyclines with or without radiation therapy.10 Thankfully, however, the 5-year survival rate remains favorable and exceeds 85%-90% for adolescents diagnosed with HL in the developed world.9
Inclusion of mediastinal/intrathoracic mass (caused by HL or other malignancy) in the differential diagnosis of children presenting with chronic cough is paramount to early identification and treatment. In its limited/early stages (stage I or II), treatment response and outcomes are excellent.8 However, without a broader consideration of etiologies, clinicians may fail to consider alternative diagnoses in patients with common complaints, such as cough, and fall prey to premature closure. Premature closure, or settling on a diagnosis quickly and without consideration for alternate causes, is a frequent cognitive bias responsible for diagnostic errors.11 Clinicians may diagnose based on their knowledge and past experiences to recognize a pattern from individual signs and symptoms—the heuristic approach—or they may rely on statistical models of likelihood—the Bayesian model.[11] Clinicians practicing in fast-paced, high-volume acute care settings like UC may are particularly prone to this cognitive error, and therefore must maintain vigilance in appropriate data gathering and creating a broad differential that accounts for the entirety of the patient’s presentation.
Like many other patients, the patient described in this case presented to the UC setting during the height of the COVID-19 pandemic and respiratory season with a cough. However, because of the chronicity of the symptom, negative viral test results, and lack of response to anti-tussive agents, the differential diagnosis was appropriately broadened, and reasonable, low-risk, further testing (ie, CXR) was performed. This ultimately demonstrated the underlying cause of the patient’s chronic cough and allowed for prompt oncological evaluation and definitive diagnosis.
Ethics Statement
The patient and parent were unable to be contacted as the phone number on file was disconnected. Patient and case details have been changed to protect patient anonymity and confidentiality.
Takeaway Points
- Cough is a common presenting chief complaint in the pediatric population, especially during the winter season. However, it is important to expand the differential diagnosis in patients with cough lasting longer than 4 weeks without improvement.
- The differential diagnosis for patients presenting to the UC setting with a chronic cough should be broadened to avoid delay in diagnosis of more severe, life-threatening pathologies, including Hodgkin lymphoma.
- When patients fail to follow the expected path of a provisional diagnosis and have multiple return visits, expanding the differential and work-up can mitigate the risk of serious diagnosis errors.
- Hodgkin lymphoma is one of the most common cancers in adolescents. It has excellent rates of cure with current therapies, particularly when diagnosed in early stages
- Clinicians practicing in UC settings must be cognizant of the possibility of falling subject to biases, such as premature closure.
Article submitted October 20, 2024; accepted November 15, 2024.
References
- [1]. Paalanne N, Honkila M, Mattila S, Pokka T, Renko M, Tapiainen T. Duration of clinical symptoms in children with acute respiratory infection. Acta Paediatrica. 2022;112(4):813-819. doi:10.1111/apa.16607
- [2]. Murgia V, Manti S, Licari A, De Filippo M, Ciprandi G, Marseglia GL. Upper respiratory tract infection-associated acute cough and the urge to cough: New Insights for Clinical Practice. Pediatric Allergy, Immunology, and Pulmonology. 2020;33(1):3-11. doi:10.1089/ped.2019.113
- [3]. Masson V, Kier C, Chandran L. Cough conundrums: A guide to chronic cough in the pediatric patient. Pediatrics In Review. 2022;43(12):691-703. doi:10.1542/pir.2021-005398
- [4]. Kasi AS, Kamerman-Kretzmer R. Cough. Journal of the American Academy of Pediatrics. 2019;40(4):157-167. doi:10.1542/pir.2018-0116
- [5]. Marseglia GL, Manti S, Chiappini E, et al. Acute cough in children and adolescents: A systematic review and a practical algorithm by the Italian Society of Pediatric Allergy and Immunology. Allergol Immunopathol (Madr). 2021;49(2):155-169. Published 2021 Mar 1. doi:10.15586/aei.v49i2.45
- [6]. Alsubaie H, Al-Shamrani A, Alharbi AS, Alhaider S. Clinical practice guidelines: Approach to cough in children: The official statement endorsed by the Saudi Pediatric Pulmonology Association (SPPA). Int J Pediatr Adolesc Med. 2015;2(1):38-43. doi:10.1016/j.ijpam.2015.03.001
- [7]. Chang AB, Oppenheimer JJ, Weinberger MM, et al. Use of management pathways or algorithms in children with chronic cough. Chest. 2017;151(4):875-883. doi:10.1016/j.chest.2016.12.025
- [8]. Belsky JA, Hochberg J, Giulino-Roth L. Diagnosis and management of hodgkin lymphoma in children, adolescents, and young adults. Best Practice & Research Clinical Haematology. 2023;36(1):101445. doi:10.1016/j.beha.2023.101445
- [9]. Kahn JM, Kelly KM. Adolescent and young adult hodgkin lymphoma: Raising the Bar Through Collaborative Science and Multidisciplinary Care. Pediatric Blood & Cancer. 2018;65(7). doi:10.1002/pbc.27033
- [10]. Munir F, Hardit V, Sheikh IN, et al. Classical hodgkin lymphoma: From past to future—a comprehensive review of pathophysiology and therapeutic advances. International Journal of Molecular Sciences. 2023;24(12):10095. doi:10.3390/ijms241210095
- [11]. Kumar B, Kanna B, Kumar S. The pitfalls of premature closure: Clinical decision-making in a case of aortic dissection. Case Reports. 2011;2011(oct03 1). doi:10.1136/bcr.08.2011.4594
Author Affiliation: Daniel Moscato, MS, PA-C, PM Pediatric Care in Massapequa, New York and New York Institute of Technology. Joshua W. Russell, MD, Legacy-GoHealth Urgent Care, University of Chicago Pritzker School of Medicine, Journal of Urgent Care Medicine. Authors have no relevant financial interests with any ineligible companies.
Download the Article PDF: Uncovering the Unexpected: A Case of Chronic Cough in an Adolescent with an Unusual Etiology
