Published on
Urgent Message: It’s important to recognize the difference between a proximal 5th metatarsal fracture of the tuberosity alone and a proximal metaphyseal fracture, commonly referred to as a “Jones fracture.” A Jones fracture requires full immobilization with urgent surgical referral.
Michael B. Weinstock, MD; Kelly Moore, BS
Citation: Weinstock M, Moore K. Urgent Care Evaluation and Management Of Proximal 5th Metatarsal Fractures. J Urgent Care Med. 2024 18(7):25-28
Editors’ Note: While the images presented here are authentic, the patient case scenarios are hypothetical.
Clinical Scenario
A previously healthy 46-year-old man presents to the urgent care 3 hours after injuring his right foot while playing basketball. He landed while his foot was plantarflexed and inverted. He complains of pain over the lateral ankle and foot, but he can walk. He denies any paresthesias or numbness as well as pain in the midfoot, lower leg, or knee.
On exam, the patient’s vitals are normal, and he’s in no distress. He can bear some weight but walks with antalgia favoring the injured leg. The right ankle is swollen laterally with ecchymoses and there is tenderness to palpation over the lateral malleolus and the proximal 5th metatarsal. There is no pain with palpation of the knee joint, medial malleolus, or the midfoot. The patient does not tolerate laxity testing. The skin is intact, and sensation and pulses are normal.
An x-ray (XR) is performed which demonstrates a fracture of the proximal 5th metatarsal bone (Image 1).
Note that the fracture line extends through the tuberosity but does not involve the metaphysis or proximal diaphysis.
Relevant Anatomy
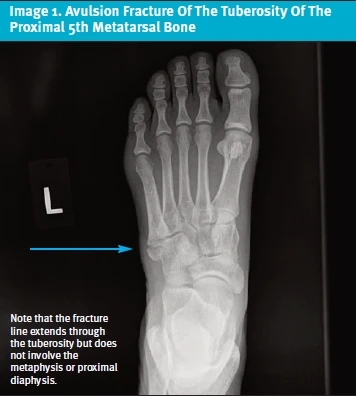
The 5th metatarsal is divided into five zones (Image 2-3). From proximal to distal, these are:
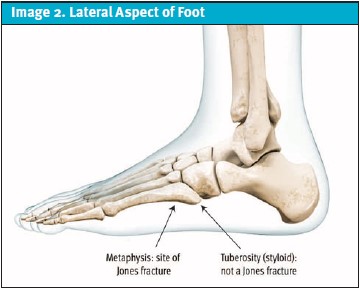
- Tuberosity (also known as “styloid”)
- Metaphysis (widened area where articulation with the cuboid and 4th metatarsal occur)
- Proximal diaphysis (elongated, narrow aspect)
- Neck
- Head
The vascular supply of the proximal 5th metatarsal arises from the metaphyseal arteries. The diaphysis is supplied by the nutrient artery.
A proximal 5th metatarsal fracture can be divided into 3 distinct categories based upon the anatomic location of the fracture (Image 1):
- Tuberosity (avulsion fracture)
- Metaphysis (Jones fracture)
- Proximal diaphysis (site of a “dancer’s fracture”)
The primary differentiation is an avulsion fracture (ie, isolated tuberosity fracture) from a metaphyseal fracture—also known as “Jones fracture” (Image 4).
A Jones fracture consists of a fracture through the metaphysis.1 This was originally described by British surgeon Sir Robert Jones in 1902 who reported on 4 patients—one of whom was actually himself—who had sustained injuries to the proximal 5th metatarsal.2 While not the case for each of these original patients, in modern usage, the term “Jones fracture” is reserved for fractures through the metaphysis, rather than avulsion fractures isolated to the proximal tuberosity (Image 1).
To avoid confusion, we suggest avoiding the use of eponyms and recommend describing the fracture site (eg, proximal metaphyseal vs. tuberosity avulsion fracture).

Note that the fracture line extends through metaphysis (the tuberosity is intact)
History
A Jones fracture is typically sustained after a twisting injury or landing after a jump, whereas the most common presentation of an avulsion fracture of the proximal 5th metatarsal tuberosity occurs with sudden pain after inversion and supination injury of the foot.3 The patient in the above scenario presented with pain over the lateral ankle and foot. Clinicians are encouraged to inquire about pain proximal and distal to this site and obtain details regarding the ankle pain itself. Without a history of an acute trauma, the differential may be expanded to include additional considerations for lateral foot pain such as chronic stress fracture, which commonly occur at the proximal diaphysis and present with a more gradual onset of pain. Non-traumatic causes for foot pain that might be considered include septic arthritis, cellulitis, and gout.
Physical Examination
Physical exam should focus on the affected lower extremity. It is important to expose and examine the entire lower leg, from the distal femur to the toes. Any swelling, erythema, ecchymosis, or tenting of the skin is important to note. Ensure the skin is intact and there are no wounds. Palpate the foot for specific areas of tenderness as well as the entire ankle, lower leg, and knee. Significant swelling and tenderness of the midfoot is concerning for a more significant injury such as a Lisfranc fracture or dislocation. Clinicians are encouraged to assess gait and the ability to bear weight as well. Assess and document neurovascular status. If there is a question as to anatomy specific to the individual, consider examining the contralateral foot.
Though our hypothetical patient had foot pain and not ankle pain, following is a review of the Ottawa Ankle Rule:
The Ottawa Ankle Rule (OAR) was created to determine which patients with ankle injuries could have fractures excluded without imaging. If any of the following criteria are present, it is recommended to obtain a radiograph:
- Inability to bear weight both at the time of the injury and at the time of clinician evaluation (ie, inability to walk four steps or to bear weight on the affected ankle)
- Tenderness at the posterior edge or tip of lateral malleolus
- Tenderness at the posterior edge or tip of medial malleolus
The OAR has been shown to decrease the use of imagingand has been validated in multiple different patient populations and settings.4,5
Testing
Differentiation between a tuberosity avulsion fracture and a proximal metaphyseal fracture (ie, Jones fracture) is the most critical assessment in urgent care. Avulsion fractures are generally managed conservatively, whereas proximal metaphyseal fractures benefit from referral to an orthopedic surgeon or podiatrist. Image 1 demonstrates an avulsion fracture of the tuberosity where the fracture line extends through the tuberosity only and not through the metaphysis. Image 4, on the other hand, demonstrates a proximal metaphyseal fracture where the fracture line extends through the metaphysis and typically reaches the 4th metatarsal. If there are equivocal findings, comparison to an x-ray of the uninjured foot may be helpful.
Indications for Referral to the ED
- Open fracture
- Concern for Lisfranc injury
- Concern for acute compartment syndrome of the foot
- Uncontrolled pain or neurovascular compromise (commonly associated with compartment syndromes)6
- Concern for dislocation/need for immediate reduction
Management
For the UC clinician, the initial management of all 5th metatarsal fracture will be analgesia, ice, and elevation. Immobilization is also important but will differ based on the fracture type involved.
- Avulsion Fractures of the Tuberosity
Immobilization with a hard-soled shoe or walking boot is generally adequate for these fractures. Early ambulation as tolerated immediately after the injury with protected and judicious, non-impact weightbearing is recommended for those with avulsion fractures. Shorter periods of non-weightbearing and immobilization after injury have been found to be associated with reduction in pain and improved functional benefits.7,8 Analgesia and crutches may also be used for pain management and comfort. Consideration of referral to orthopedics or podiatry is appropriate, but initial follow-up with primary care is also reasonable depending on the practice setting. - Metaphyseal or Proximal Diaphyseal Fracture (ie, Jones Fracture)
For those with more distal fractures involving the metaphysis or proximal diaphysis, patients should be immobilized in a splint and instructed to use crutches and remain non-weight bearing until follow up with an orthopedic surgeon.3 Patents with more distal fractures of the 5th metatarsal (ie, beyond the tuberosity) benefit from specialist referral to either an orthopedic surgeon, podiatrist, or other appropriate surgical specialist for re-evaluation and consideration for possible surgery. Early surgical fixation of such fractures results in lower rates of non-union and faster time to healing compared to conservative management.9 In one study, surgical fixation also resulted in a faster return to sports of 2 months with early screw fixation compared to casting.10
Next-Level Urgent Care Pearls
- Ask about prodromal symptoms. A stress fracture manifests over time. A true proximal 5th metaphyseal fracture (ie, Jones) is from acute trauma without prodromal symptoms.10
- An accessory ossicle bone may be confused with a fracture of the proximal 5th metatarsal. These ossicles are typically round in contour, compared with a fracture, which is typically irregular and jagged.
- Features present with nonunion may include: repetitive trauma; recurrent symptoms; and a wide fracture line with new bone evident but remaining radiolucent.
Red Flags and Legal Pitfalls
- Evaluate for other injuries involving the other extremities, head, and/or neck.
- Examine the joint proximal and distal to the area of greatest pain.
- Palpate the proximal fibula with consideration for a Maisonneuve fracture (ie, spiral fracture of the proximal fibula) which can be seen with severe twisting ankle/foot injuries that affect the syndesmosis.
- Consider the possibility of the most time sensitive diagnoses with each patient with foot pain, notably compartment syndrome, necrotizing soft tissue infection, and septic arthritis.
- Ensure to document intact skin and a thorough neurovascular status assessment (eg, “the foot is warm with strong pulses and normal sensation throughout”).
Clinical Scenario Conclusion
The hypothetical patient’s XR shows an avulsion fracture of the tuberosity without involvement of the metaphysis. He’s placed in a hard-soled shoe and instructed to ambulate and bear weight as tolerated with referral to follow-up with his primary care physician in about 2 weeks. Ultimately, he should be able to return to sports in about 6 weeks post-injury.
Take Home Points
- A proximal 5th metatarsal fracture of the tuberosity alone (ie, avulsion fracture) is managed with a hard-soled shoe or walking boot and early weight bearing as tolerated. It rarely requires operative intervention.
- A proximal metaphyseal fracture, commonly referred to as a “Jones fracture,” requires full immobilization with a below the knee splint and non-weight bearing status with urgent surgical referral as such fractures have a high rate of non-union without fixation.
- If not confident about which fracture pattern is present and immediate specialist/radiologist confirmation is not available, it is prudent to err on the side of full immobilization, prohibition of weightbearing, and urgent specialist referral.
Manuscript submitted January 3, 2024; accepted February 24, 2024.
References
- Metzl JA, Bowers MW, Anderson RB. Fifth Metatarsal Jones Fractures: Diagnosis and Treatment. J Am Acad Orthop Surg. 2022;30(4):e470-e479. doi:10.5435/JAAOS-D-21-00542
- Jones R. Fractures of the base of the fifth metatarsal bone by indirect violence. Ann Surg. 1902;35:697-702
- Porter DA, Klott J. Proximal Fifth Metatarsal Fractures in Athletes: Management of Acute and Chronic Conditions. Foot Ankle Clin. 2021;26(1):35-63. doi:10.1016/j.fcl.2020.10.007
- Gomes YE, Chau M, Banwell HA, Causby RS. Diagnostic accuracy of the Ottawa ankle rule to exclude fractures in acute ankle injuries in adults: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2022;23(1):1-11.
- Dowling S, et al. Accuracy of Ottawa ankle rules to exclude fractures of the ankle and midfoot in children: a meta-analysis. Acad Emerg Med. 2009;16(4):277–287
- Marchesi M, Marchesi A, Calori GM, et al. A sneaky surgical emergency: Acute compartment syndrome. Retrospective analysis of 66 closed claims, medico-legal pitfalls and damages evaluation. Injury. 2014;45 Suppl 6:S16-S20. doi:10.1016/j.injury.2014.10.017
- Bowes J, Buckley R. World J Orthop. 2016;7(12):793-800. doi:10.5312/wjo.v7.i12.793
- Vorlat P, Achtergael W, Haentjens P. Predictors of outcome of non-displaced fractures of the base of the fifth metatarsal. Int Orthop. 2007;31(1):5-10. doi:10.1007/s00264-006-0116-9
- Rikken QGH, Dahmen J, Hagemeijer NC, Sierevelt IN, Kerkhoffs GMMJ, DiGiovanni CW. Adequate union rates for the treatment of acute proximal fifth metatarsal fractures. Knee Surgery, Sport Traumatol Arthrosc. 2021;29(4):1284-1293.
- Mologne TS, et al. Early screw fixation versus casting in the treatment of acute Jones fractures. Am J Sports Med. 2005; 33:970-975.
Read More
- A 16-Year-Old With Severe Pain And Immobility After A Basketball Mishap
- Managing Foot Fractures In Urgent Care
- An Unusual Case Of Third And Fourth Metacarpophalangeal Joint Dislocations Following A Fall
